

Background
IgM paraprotein-associated peripheral neuropathies (PN) are a heterogenous group of disorders seen in patients with IgM MGUS and Waldenström's Macroglobulinaemia (WM). Anti-myelin associated glycoprotein (MAG) antibodies are causally identified in ~50% of such cases, but other neuropathies with other IgM-targets are described, along with AL amyloidosis and cryoglobulinaemic vasculitis amongst others. Presence of neuropathy alone is typically not an indication for treatment, but progressive disability is. Due to their relative rarity and heterogeneity, the true prevalence and optimal management of these neuropathies is currently unclear.
Methods
The Rory Morrison WMUK Registry, a national IgM-related disorders database incorporating 18 centres, was searched for all patients with PN and retrospective data clinical data extracted. Research ethics approval was obtained.
Results
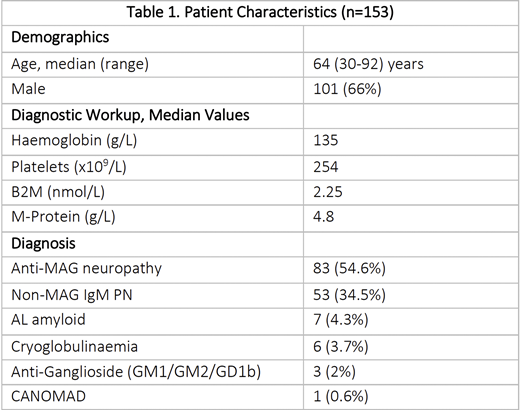
IgM-related PN was identified 153 patients, of whom 99 (64.7%) had underlying WM and 54 (35.3%) had IgM MGUS. Anti-MAG neuropathy was present in 83 (54.6%) patients, anti-ganglioside in 3 (2%), AL amyloid in 7 (4.3%), cryoglobulinemia in 6 (3.7%), one (0.6%) case of CANOMAD syndrome, and a non-MAG IgM-neuropathy in 53 (34.5%%). PN was present at diagnosis in 143 (93.5%) whereas 10 (6.5%) were diagnosed during the course of their disease.
Median age at diagnosis was 64 years (30-92) and 101/153 (66%) were male. Table 1 details results at diagnosis. κ-light chain was present in 80.3%, λ in 11.8% and 7.9% had multiple M-protein bands expressing both light chains. MYD88L265P was identified in 44/55 tested patients (80%) and in 23/30 (76.7%) cases of anti-MAG. In those with an IgM-related disorder, 13/20 (65%) had MYD88L265P, higher than in other IgM MGUS patients (7/14, 50%). CXCR4MUT were found in 3/22 (13.6%). Median bone marrow infiltration on trephine was 13% (range 0-85%), but 10 patients had no evidence of disease, 5 had disease on flow cytometry only, 2 an isolated finding of MYD88L265P and 1 isolated CXCR4MUT on PCR. IgM-related PN was seen in 99/719 (13.8%) of all registry patients with WM. At diagnosis, the bone marrow burden, M-protein and B2M were all significantly lower (p<0.001) than in those with WM without PN, despite identical median age.
Therapy had been required in 81 (53.3%) patients, including at time of diagnosis in 23 (15%). Median time from diagnosis to treatment was long, at 6.7 years (95% CI 3.2-9.1 years). PN was the sole treatment indication in 64/81 (79%) cases. Time to treatment commencement did not appear to be affected by M-protein quantity or marrow burden, but patients with WM were more likely to have received treatment for their PN (59/108, 54.6%). Frontline treatment incorporated rituximab (R) in 66/81 (81.5%) patients, including R-monotherapy in 30, DRC 20, R-CHOP/R-CVP eight and BR in seven. A major biochemical response was seen in 19/34 (55.9%) patients. Clinical response was seen in 34 of 45 evaluable cases (75.6%), with improvement in 13 (28.9%) and stabilisation in 21 (46.7%). Clinical response or stabilisation was significantly more likely with R-containing therapy (82.1% vs 33.3%, p 0.04), non-amyloid related PN (82% vs 0%, p = 0.01) and attainment of ≥ partial response. All patients (n=12) with normal BMAT or isolated MYD88L265P responded to R-containing frontline therapy, another positive prognostic factor (p = 0.08).
Progression of PN occurred after an initiation period of clinical response in 7/34 (20.5%), necessitating re-treatment at a median of 4.3 years after frontline therapy. Median time to 2nd line therapy was 6.7 years, longer than for other WM treatment indications (p = 0.04).
Conclusions
IgM-related PN is a cause of morbidity for a significant proportion of patients with WM, with a prevalence of 13.7%. However, a third of cases occur in those with IgM MGUS and even very small clonal populations seem capable of causing disease but appear responsive to rituximab therapy. Patients typically have comparatively low systemic disease burden and low rates of CXCR4MUT, perhaps representing a more indolent phenotype or a product of earlier diagnosis. PN is frequently the sole indication for treatment, reflecting this. Clinical improvement or stabilisation was seen in 75% of treated patients, and attainment of ≥50% reduction in IgM (PR) and treatment with rituximab is associated with a more favourable outcome, whereas AL amyloid neuropathy appears to be more treatment resistant.
Lindsay:Amgen: Other: Travel Expenses; Takeda: Honoraria, Other: Travel Expenses; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel Expenses. Carr:Lupin: Honoraria; CSL: Honoraria; Grifols: Other: Travel support. McCarthy:Janssen: Honoraria; Abbvie: Membership on an entity's Board of Directors or advisory committees. El-Sharkawi:Roche: Other: Conference fees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees. Pratt:Binding Site Ltd: Other: Personal fees; Amgen: Other: Personal fees; Janssen: Other: Personal fees; Celgene: Other: Personal fees; Takeda: Other: Personal fees; Gilead: Other: Personal fees; Sanofi-Genzyme: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Beigene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Karyopharm: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding. D'Sa:Janssen: Honoraria, Research Funding; Sanofi: Honoraria; BeiGene: Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal