

Introduction
The antibody-drug conjugate polatuzumab vedotin (Pola) has recently been approved in combination with bendamustine and rituximab (Pola-BR) for patients with r/r diffuse LBCL (DLBCL).
Methods
To characterize the efficacy of Pola-BR in a real-world setting, we retrospectively analyzed data from 97 patients with r/r LBCL who were treated with Pola in 24 German centers within the national CUP. Clinical baseline and follow-up (FU) data were collected by chart review and summarized descriptively. Progression-free survival (PFS) and overall survival (OS) were analyzed using Kaplan-Meier and Cox regression methods. Fisher's exact test was used to compare categorical factors between groups of patients.
Results
97 patients with LBCL (DLBCL n=90, High-grade B-cell lymphoma n=6, Primary mediastinal B-cell lymphoma n=1) were included as of July 22nd, 2020. 49 patients were treated with Pola as bridging concept to immunotherapies (bridging cohort: chimeric antigen receptor T-cells (CART) n=39, allogeneic stem cell transplantation (alloSCT) n=9, bispecific antibodies n=1), and 48 patients were treated with Pola in palliative intention (palliative cohort).
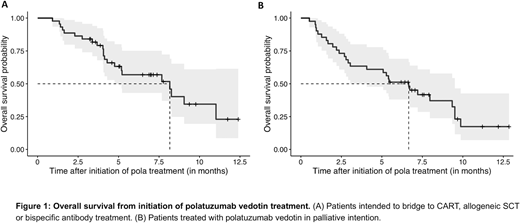
Within the bridging cohort the median age was 61 years (range: 22-82). Patients were heavily pretreated with a median of 3 treatment lines (range: 2-6). 84% (41/49 patients) had been refractory to their last treatment line, and 31% had failed an autologous stem cell transplantation. Notably, 14% and 10% of patients had failed prior CART and alloSCT, respectively, and were planned for the alternate cellular immunotherapy. Based on an individual decision, patients were treated with Pola-Rituximab (Pola-R, n=20), Pola-chemotherapy (Pola-chemo, BR n=25; R-CHP n=1) or Pola-monotherapy (Pola-mono, n=3). With a median of 2 Pola cycles (range 1-6), overall response rate (ORR) of all evaluable patients was 33% (15/46 patients) including patients with complete response (CR n=1), partial response (PR n=9) and clinical response (n=5). Although not significant, ORR tended to be better in patients treated with Pola-chemo versus Pola-R/Pola-mono (ORR: 42% versus 20%, Fishers test p=0.1). 11 of these 15 responders (24% of the entire bridging cohort) proceeded to CART or alloSCT, while 4 responders (8% of entire bridging cohort) experienced fast progression after their initial response and were referred to best supportive care. 15 of 31 non-responders (33% of entire bridging cohort) underwent immunotherapy with either stable disease (n=6), mixed response (n=2), or progression on Pola (n=7). The remaining 16 patients (35% of entire bridging cohort) were all refractory to Pola and either received alternative salvage treatments which enabled 8 further patients to proceed to the intended immunotherapy, or best supportive care. Taking the effects of CART or alloSCT into account, median OS from initiation of Pola treatment was 8.2 months (median FU 7.2 months, Fig. 1A).
The palliative cohort tended to be older than the bridging cohort with a median age of 73.5 years (range: 37-86, p<0.001). Patients were pretreated with a median of 3 treatment lines (range: 2-8), and 85% (41/48 patients) had been refractory to their last treatment line. Patients in the palliative cohort were treated with a median of 4 Pola cycles (range: 1-9). 65% received Pola-chemo (BR, n=30; R-Gemcitabine, n=1) and 35% Pola-R. The CR rate and ORR was 19% (9/48) and 56% (27/48), respectively. The 6-month PFS and OS from initiation of Pola was 36% and 51%, respectively (median FU of 9.7 months, Fig. 1B). Again, ORR and OS tended to be better in patients treated with Pola-chemo versus Pola-R (ORR: 61% versus 47%, Fishers test p=0.4; median OS 7.2 versus 4 months, HR 0.8, 95%CI 0.4-1.9, p=0.7). In univariate analysis, failure to respond to the last treatment line predicted inferior PFS (HR 2.4, 95%CI 1.2-5.0 p=0.02) and OS (HR 2.5, 95%CI 1.2-5.4 p=0.02). Patients with more than two prior treatment lines in total tended to have a shorter PFS (HR 2.0, 95% CI 0.9-4.5, p=0.1) and OS (HR 1.8, 95% CI 0.8-4.0, p=0.2), although significance was not reached.
Conclusion
Pola permits effective bridging to CART and alloSCT in r/r LBCL. In the palliative setting, Pola represents an effective salvage option for patients with transplantation-ineligible r/r LBCL. Compared to the approval study, the inferior outcome of the patients of this real-world analysis might be explained by their more advanced disease course.
Duell:Morphosys: Research Funding. Kerkhoff:BMS: Honoraria. Leng:Roche: Other: lecture fee; Celgene: Other: traveling expenses and congress attendance fee. Holtick:Miltenyi Biotec B.V. & Co. KG: Honoraria. Mayer:Amgen: Honoraria, Other: travel grants; Abbvie: Other: travel grants; Novartis: Honoraria; Roche: Honoraria. Hüttmann:Celgene: Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company); Gilead: Honoraria; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company); Roche: Other: Travel expenses; Seattle Genetics: Research Funding; University Hospital Essen, University of Duisburg-Essen, Essen, Germany: Current Employment; Lead Discovery Center GmbH: Consultancy. Brunnberg:Gilead: Membership on an entity's Board of Directors or advisory committees; Hexal: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Other: travel grants; MSD: Membership on an entity's Board of Directors or advisory committees; Roche: Membership on an entity's Board of Directors or advisory committees, Other: Travel grants; Amgen: Other: Travel grants. Bullinger:Menarini: Membership on an entity's Board of Directors or advisory committees; Gilead: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees; Daiichi Sankyo: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; Hexal: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees; Sanofi: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; Bristol-Myers Squibb: Membership on an entity's Board of Directors or advisory committees. Hess:Roche: Research Funding; Celgene: Research Funding; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Genmab: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Astra: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; EUSA: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Morphosys: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Mueller-Tidow:Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding; Deutsche Krebshilfe: Research Funding; BMBF: Research Funding; Wilhelm-Sander-Stiftung: Research Funding; Jose-Carreras-Siftung: Research Funding; Bayer AG: Research Funding; Daiichi Sankyo: Research Funding; BiolineRx: Research Funding; Janssen-Cilag Gmbh: Membership on an entity's Board of Directors or advisory committees; Deutsche Forschungsgemeinschaft: Research Funding. Lenz:Verastem: Research Funding; AQUINOX: Research Funding; BMS: Consultancy; AstraZeneca: Consultancy, Honoraria, Research Funding; Bayer: Consultancy, Honoraria, Research Funding, Speakers Bureau; Agios: Research Funding; Gilead: Consultancy, Honoraria, Research Funding, Speakers Bureau; Roche: Consultancy, Honoraria, Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Speakers Bureau; Novartis: Consultancy; Morphosys: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau. Dreger:Roche: Consultancy, Speakers Bureau; Neovii: Research Funding; AbbVie: Consultancy, Speakers Bureau; AstraZeneca: Consultancy; Gilead: Consultancy, Speakers Bureau; Janssen: Consultancy; Novartis: Consultancy, Speakers Bureau; Riemser: Consultancy, Research Funding, Speakers Bureau. Dietrich:Roche: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; KITE: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal