

Background:
DNA-hypomethylating agents are providing a very well-accepted backbone for non-intensive combination treatment of AML/MDS patients (pts), and an in vivo synergism has been demonstrated for the azacitidine+venetoclax combination in the VIALE-A trial (DiNardo et al., EHA 2020). The DAC+ATRA combination also resulted in an improved response rate and survival compared to DAC without ATRA (DECIDER trial, Lübbert et al., J. Clin. Oncol. 2020), also in pts with prior hematologic disorder (mostly MDS); no benefit was seen when valproic acid (VPA) was added to DAC (2x2 factorial design). In a previous study, we had investigated the outcome of elderly pts with oligoblastic AML (i.e. with 20-30% bone marrow blasts, defined as MDS RAEBt according to the French-American-British classification) treated with either DAC or best supportive care within the EORTC 06011 phase III trial (Becker et al., Ann. Hematol. 2015), observing a median overall survival (OS) of 8.0 months (mths) in DAC-treated RAEBt pts. We now hypothesized that the outcome of pts with oligoblastic AML may be improved by the addition of ATRA to DAC. Therefore, in the present exploratory subgroup analysis, pts from the DECIDER cohort with 20-30% bone marrow blasts were analyzed for clinical outcome.
Patients and Methods:
Key inclusion criteria: newly diagnosed pts >60 years (yr), unfit for induction with non-M3 AML (WHO, de novo or after antecedent hematologic disorder [AHD], therapy-associated [t]AML), ECOG performance status (PS) 0-2. Treatment: DAC 20 mg/m2 day 1-5 (treatment arms A/B/C/D), ATRA p.o. day 6-28 (arms C/D), VPA p.o. continuously from day 6 (arms B/D), of each 28-day course (repeated until relapse/progression, prohibitive toxicity, withdrawal or death). Key endpoints: objective response rate (ORR): CR/CRi/PR, overall (OS) and event-free survival (EFS). Sample size calculation was based on the primary endpoint ORR, assuming an ORR of 25% in arm A (Lübbert et al., Haematologica 2012). For a power of 80% (test in this phase II study at 1-sided alpha=0.1) for an increase of ORR to 40% with ATRA or VPA, 176 pts were necessary, planned sample size 200. Between 12/2011 and 2/2015, 200 pts were randomized and treated. Efficacy analyses were performed in the intention-to-treat (ITT) population. ATRA was investigated by comparing arms C+D vs arms A+B, VPA by comparing arms B+D vs arms A+C, ORR was analyzed with logistic regression estimating odds ratios (OR), OS/EFS with Cox regression estimating hazard ratios (HR), each with 95% confidence intervals (CI), and presented with descriptive two-sided p values of the tests of no treatment effect. Central hematopathologic review (blinded as to treatment arms) was conducted by an independent morphologist.
Results:
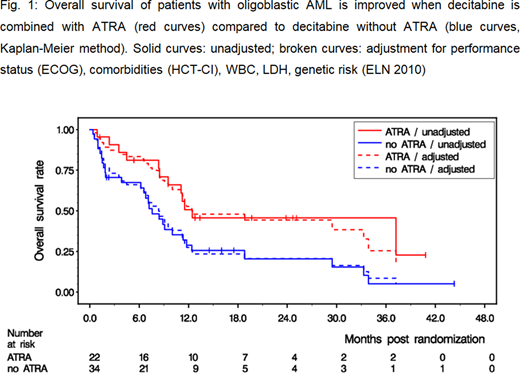
In 56/200 pts of the DECIDER cohort, bone marrow blasts were 20-30% (median, 25%). The number of pts in the randomized arms were: 13 in arm A, 21 in arm B, 9 in arm C, 13 in arm D. Baseline pt characteristics were as follows: male 77%, median age: 75 yr (range 61-88), median WBC: 3400/µl (range 500-52,600), adverse genetics (ELN 2010) present in 25%, ECOG 2 in 13%, comorbidities (HCT-CI) ≥ 3 in 48%, AHD in 68%, tAML in 11% (only slight random imbalances across randomized treatment arms). A median of 5 DAC courses were administered (per arm: 2/5/11/4). Six pts attained a CR, 7 pts a CRi, and 1 pt a PR, resulting in an ORR of 25% (arm A: 7.7%, arm B: 28.6%, arm C: 33.3%, arm D: 30.8%, respectively). Effect on ORR of ATRA vs no ATRA (31.8 vs 20.6%): OR 1.85, CI [0.54,6.37], p=0.33; and of VPA vs no VPA (29.4 vs 18.2%): OR 1.93, CI [0.51,7.24], p=0.33. With 40 deaths out of 56 pts, median OS was 9.5 mths (arm A: 7.6 mths, arm B: 8.9 mths, arm C: 37.2 mths, arm D: 11.2 mths, respectively). Effect on OS of ATRA vs no ATRA (12.5 vs 7.6 mths median OS): HR 0.47, CI [0.24,0.94], p=0.032 (after adjustment for PS, HCT-CI, WBC, LDH, genetic risk: HR 0.42, CI [0.19,0.90], p=0.025); and of VPA vs no VPA (10.0 vs 8.4 mths median OS): HR 0.99, CI [0.51,1.92], p=0.98: A comparable benefit on EFS of ATRA vs no ATRA (but not VPA vs no VPA) was observed.
Conclusion:
In elderly pts with oligoblastic AML ineligible for induction chemotherapy, the addition of ATRA, but not VPA, to DAC resulted in a clinically meaningful survival benefit; OS of pts receiving DAC without ATRA was very similar to that observed in a previous study. It is tempting to speculate that the combination of an HMA with a retinoid such as ATRA may also be active in MDS pts with excess of blasts.
Jost:JAZZ: Other: travel support; Roche: Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees; Celgene: Other: travel support. Thol:Daiichi Sankyo: Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees. Heuser:Amgen: Research Funding; Bayer: Consultancy, Research Funding; BerGenBio ASA: Research Funding; Daiichi Sankyo: Consultancy, Research Funding; Stemline Therapeutics: Consultancy; Janssen: Consultancy; PriME Oncology: Honoraria; Karyopharm: Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy; Astellas: Research Funding; Roche: Research Funding; Novartis: Consultancy, Honoraria, Research Funding. Götze:Celgene: Research Funding. Schlenk:Daiichi Sankyo: Membership on an entity's Board of Directors or advisory committees, Other: Travel, Accomodations, Expenses, Research Funding, Speakers Bureau; Novartis: Speakers Bureau; Roche: Research Funding; AstraZeneca: Research Funding; PharmaMar: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau. Döhner:Sunesis Pharmaceuticals: Research Funding; Abbvie: Consultancy; Agios: Consultancy; Amgen: Consultancy, Research Funding; Astellas Pharma: Consultancy; Bristol-Myers Squibb: Research Funding; Pfizer: Research Funding; Arog: Research Funding; Roche: Consultancy; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding; Astex Pharmaceuticals: Consultancy; Janssen: Consultancy, Honoraria; Daiichi Sankyo: Honoraria; Celgene: Consultancy, Honoraria; Novartis: Honoraria, Research Funding. Salih:Synimmune: Consultancy, Research Funding; Philogen: Consultancy; Medigene: Consultancy; Novartis: Consultancy; Pfizer: Consultancy. Schittenhelm:Pfizer: Consultancy; Astellas: Consultancy. Mueller-Tidow:Jose-Carreras-Siftung: Research Funding; Wilhelm-Sander-Stiftung: Research Funding; BMBF: Research Funding; Deutsche Krebshilfe: Research Funding; Deutsche Forschungsgemeinschaft: Research Funding; Janssen-Cilag Gmbh: Membership on an entity's Board of Directors or advisory committees; BiolineRx: Research Funding; Daiichi Sankyo: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding; Bayer AG: Research Funding. Brugger:MorphoSys: Current Employment. Bug:Jazz: Honoraria; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel; Hexal: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees; Eurocept: Membership on an entity's Board of Directors or advisory committees; Gilead: Membership on an entity's Board of Directors or advisory committees, Other: Travel; Sanofi: Other: Travel; Neovii: Other: Travel. Wäsch:Pfizer: Consultancy; Amgen: Consultancy; Janssen: Consultancy. Ganser:Celgene: Consultancy; Novartis: Consultancy. Döhner:AstraZeneca: Consultancy, Honoraria; Sunesis: Research Funding; Roche: Consultancy, Honoraria; Pfizer: Research Funding; Oxford Biomedicals: Consultancy, Honoraria; Novartis: Consultancy, Honoraria, Research Funding; Helsinn: Consultancy, Honoraria; Jazz: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Bristol Myers Squibb: Consultancy, Honoraria, Research Funding; Astex: Consultancy, Honoraria; Astellas: Consultancy, Honoraria, Research Funding; AROG: Research Funding; Amgen: Consultancy, Honoraria, Research Funding; Agios: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria; GEMoaB: Consultancy, Honoraria.
ATRA is approved for APL treatment but not for non-APL AML

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal