

Background
Polycythemia vera (PV) is a myeloproliferative neoplasm (MPN) associated with an increased risk of thrombotic events (TEs), a major cause of morbidity and mortality. Patients aged ≥60 years and/or with a history of thrombosis are considered to have high-risk PV. There is limited contemporary, real-world evidence exploring the effect of TEs on mortality in patients with PV. The aim of this analysis was to compare the risk of mortality in patients newly diagnosed with high-risk PV who experienced a TE vs those who did not experience a TE.
Study Design and Methods
All data from the Medicare Fee-for-Service (FFS) claims database (Parts A/B/D) from January 2010-December 2017 were used to identify patients with a PV diagnosis (all high risk based on cohort being ≥65 years of age) with ≥1 inpatient or ≥2 outpatient claims. The index date was the date of the first qualifying PV claim. Patients with a PV diagnosis or use of cytoreductive therapy within 12 months before the index date (pre-index period) were excluded; ≥12-months continuous medical and pharmacy enrollment pre-index dates was required. The study sample was categorized into TE and non-TE groups based on the occurrence of any of the following events during follow-up: deep vein thrombosis, pulmonary embolism, ischemic stroke, acute myocardial infarction, transient ischemic attack, peripheral arterial thrombosis, or superficial thrombophlebitis. TEs were evaluated from the index date to the end of follow-up. Cox regression analyses with time-varying effects were used to assess mortality risk among patients with PV, with post-index TE as a time-dependent variable, stratified by pre-index TE, and adjusting for patient demographic characteristics and comorbid conditions.
Results
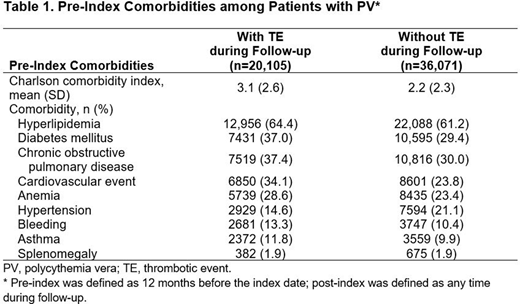
A total of 56,176 Medicare FFS beneficiaries with PV diagnoses met inclusion criteria. The median age was 73 years, 51.9% were men, and 90.7% were white; 10,110 patients (18.0%) had a history of TE before diagnosis (ie, pre-index). In the follow-up period, 20,105 patients (35.8%) had a TE and 36,071 patients (64.2%) did not have a TE. In the comparison between the TE vs non-TE groups, the median (range) age (75.0 [65-104] vs 73.0 [65-106] years, respectively), mean (SD) Charlson comorbidity index score (3.1 [2.6] vs 2.2 [2.3]), and percentage of patients with a history of cardiovascular events (34.1% vs 23.8%), bleeding (13.3% vs 10.4%), or anemia (28.6% vs 23.4%) were higher (Table 1).
Among all patients with PV, the median time from diagnosis to first post-index TE was 7.5 months. Among those with pre-index TE (n=10,093), median time from index to first post-index TE was 0.6 months, whereas patients without pre-index TE (n=46,083) had a median time to first post-index TE of 14.2 months. Among all patients with TE during follow-up, the most common TEs were ischemic stroke (47.5%), transient ischemic attack (30.9%), and acute myocardial infarction (30.5%).
The risk of mortality was increased for patients who experienced a TE compared with those who did not (hazard ratio [HR; 95% CI], 9.3 [8.4-10.2]; P<0.0001). For patients who experienced a pre-index TE, the risk of mortality was increased for patients who experienced a subsequent TE during follow-up compared with patients who did not (HR [95% CI], 6.7 [5.8-7.8]; P<0.0001). Likewise, for patients who did not experience a pre-index TE, the risk of mortality was increased for patients who experienced a TE during follow-up compared with patients who did not (HR [95% CI], 13.1 [11.4-15.0]; P<0.0001).
Conclusions
In this real-world study, approximately one-third of patients with newly diagnosed high-risk PV experienced a TE during follow-up and had a 9-fold increased risk of mortality vs those who did not experience a TE. TE risk mitigation remains an important management goal in patients with PV, particularly in those with prior TE.
Pemmaraju:Samus Therapeutics: Research Funding; Celgene: Honoraria; SagerStrong Foundation: Other: Grant Support; Affymetrix: Other: Grant Support, Research Funding; MustangBio: Honoraria; Blueprint Medicines: Honoraria; LFB Biotechnologies: Honoraria; Plexxikon: Research Funding; Novartis: Honoraria, Research Funding; AbbVie: Honoraria, Research Funding; Stemline Therapeutics: Honoraria, Research Funding; Pacylex Pharmaceuticals: Consultancy; Daiichi Sankyo: Research Funding; Incyte Corporation: Honoraria; Roche Diagnostics: Honoraria; Cellectis: Research Funding; DAVA Oncology: Honoraria. Gerds:Sierra Oncology: Research Funding; Celgene: Consultancy, Research Funding; Gilead Sciences: Research Funding; Imago Biosciences: Research Funding; Pfizer: Research Funding; CTI Biopharma: Consultancy, Research Funding; Roche/Genentech: Research Funding; Apexx Oncology: Consultancy; AstraZeneca/MedImmune: Consultancy; Incyte Corporation: Consultancy, Research Funding. Parasuraman:Incyte Corporation: Current Employment, Current equity holder in publicly-traded company. Yu:Incyte Corporation: Current Employment, Current equity holder in publicly-traded company. Shah:Avalere Health: Current Employment. Xi:Incyte Corporation: Other: Avalere Health is a paid consultant of Incyte Corporation; Avalere Health: Current Employment. Kumar:Avalere Health: Current Employment; Incyte Corporation: Other: Avalere Health is a paid consultant of Incyte Corporation. Scherber:Incyte Corporation: Current Employment, Current equity holder in publicly-traded company. Verstovsek:Gilead: Research Funding; Incyte Corporation: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; CTI Biopharma Corp: Research Funding; Promedior: Research Funding; Roche: Research Funding; AstraZeneca: Research Funding; Blueprint Medicines Corp: Research Funding; Genentech: Research Funding; Sierra Oncology: Consultancy, Research Funding; Protagonist Therapeutics: Research Funding; ItalPharma: Research Funding; PharmaEssentia: Research Funding; NS Pharma: Research Funding; Celgene: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal