

Serum protein electrophoresis/immunofixation electrophoresis (SPEP/IFE) was performed on a 63-year-old woman with a history of Waldenstrom macroglobulinemia, on ibrutinib, and identified the known monoclonal immunoglobulin M λ paraprotein (*, panels A-C), at 0.3 g/dL. In addition, a faint cathodal immunoglobulin G (IgG) κ monoclonal protein was identified (↔, panel C) by IFE. At the time, the patient was admitted to the hospital with acute hypoxemic respiratory failure and was subsequently diagnosed with persistent acute COVID-19 infection. Two months before admission, she developed a cough and sore throat, tested positive for COVID-19, and received sotrovimab, an IgG κ COVID-19 monoclonal antibody (MAb) therapy. Given the patient’s history of Waldenstrom macroglobulinemia, SPEP/IFE was sent during admission, to exclude hyperviscosity as a contributor to the patient’s dyspnea. The faint IgG κ monoclonal band was interpreted as evidence of the patient’s prior COVID-19 MAb therapy. The patient was discharged 1 month after admission, in stable condition, on 1 L of oxygen and a prednisone taper.
MAb therapies, which are typically IgG κ type, are commonly used for the treatment of B-cell lymphoma and multiple myeloma, and now COVID-19 infection. Pathologists and clinicians must be aware that nondisease-associated, therapeutic MAbs can be identified by serum IFE. This case demonstrates that a thorough evaluation of patient history is required to avoid overinterpretation of new monoclonal IgG κ bands identified by SPEP/IFE.
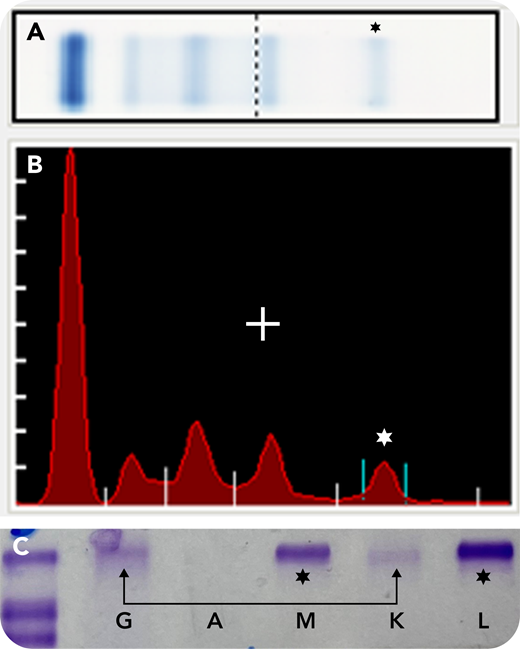
Serum protein electrophoresis/immunofixation electrophoresis (SPEP/IFE) was performed on a 63-year-old woman with a history of Waldenstrom macroglobulinemia, on ibrutinib, and identified the known monoclonal immunoglobulin M λ paraprotein (*, panels A-C), at 0.3 g/dL. In addition, a faint cathodal immunoglobulin G (IgG) κ monoclonal protein was identified (↔, panel C) by IFE. At the time, the patient was admitted to the hospital with acute hypoxemic respiratory failure and was subsequently diagnosed with persistent acute COVID-19 infection. Two months before admission, she developed a cough and sore throat, tested positive for COVID-19, and received sotrovimab, an IgG κ COVID-19 monoclonal antibody (MAb) therapy. Given the patient’s history of Waldenstrom macroglobulinemia, SPEP/IFE was sent during admission, to exclude hyperviscosity as a contributor to the patient’s dyspnea. The faint IgG κ monoclonal band was interpreted as evidence of the patient’s prior COVID-19 MAb therapy. The patient was discharged 1 month after admission, in stable condition, on 1 L of oxygen and a prednisone taper.
MAb therapies, which are typically IgG κ type, are commonly used for the treatment of B-cell lymphoma and multiple myeloma, and now COVID-19 infection. Pathologists and clinicians must be aware that nondisease-associated, therapeutic MAbs can be identified by serum IFE. This case demonstrates that a thorough evaluation of patient history is required to avoid overinterpretation of new monoclonal IgG κ bands identified by SPEP/IFE.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal