Key Points
Patients with acute leukemia present with a prolonged and severe course of COVID-19, which is paralleled by high rates of viremia.
Low-intensive chemotherapy seems to be more feasible in patients with acute myeloid leukemia and concomitant SARS-CoV-2 infection.

Introduction
Since January 2020, >30 million cases of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections have been confirmed globally.1 Yet, there is almost no information on the clinical impact of coronavirus disease 2019 (COVID-19) in adults with acute leukemia (AL). Because untreated newly diagnosed or refractory/relapsed AL is fatal, these patients require immediate chemotherapy in spite of concomitant SARS-CoV-2 infection. We report a series of 12 patients with AL and SARS-CoV-2 infection who were treated in our department between 18 March and 18 May 2020.
Case description
Eight patients (67%) had acute myeloid leukemia (AML); 4 patients (33%) had acute lymphoblastic leukemia (ALL) or lymphoblastic lymphoma (LBL).
Characteristics of AML patients
At SARS-CoV-2 diagnosis, 3 patients had untreated, newly diagnosed AML; 4 patients had refractory/relapsed AML. One patient was in complete remission with incomplete hematologic recovery (CRi) and received high-dose cytarabine for consolidation. All 4 refractory/relapsed patients had been treated with intensive chemotherapy before SARS-CoV-2 confirmation. After SARS-CoV-2 infection, 6 patients received therapy with azacytidine and venetoclax2 ; 1 patient with newly diagnosed AML received induction therapy with daunorubicin and cytarabine (3+7).
Clinical course of AML patients
The only AML patient who was in remission started 12 days after SARS-CoV-2 diagnosis with high-dose cytarabine consolidation therapy. He died 23 days after SARS-CoV-2 infection due to severe acute respiratory distress syndrome (ARDS) despite extracorporeal membrane oxygenation (ECMO) in deep aplasia. All three AML patients with newly diagnosed AML developed severe ARDS: the only one who was treated with intensive chemotherapy died. None of the 4 refractory AML patients treated with azacytidine/venetoclax developed ARDS.
Characteristics of ALL patients
One patient had newly diagnosed untreated Philadelphia chromosome–positive common B-cell ALL (B-ALL) and received prephase treatment 5 days before SARS-CoV-2 infection, and continued with induction therapy. Three patients were already under ALL-specific treatment at SARS-CoV-2 diagnosis: 1 elderly patient with T-cell ALL (T-ALL) received induction therapy. The patient with T-cell LBL (T-LBL) in complete remission after induction and consolidation therapy received 1 course of reinduction therapy. One minimal residual disease–positive patient with B-ALL received continuous infusion of blinatumomab (for patients characteristics, see Table 1). All ALL patients were treated according to recommendations of the German Multicenter Study Group on Adult ALL (NCT number 02881086).
Clinical course of ALL/LBL patients
One patient with newly diagnosed ALL developed severe ARDS and deep vein thrombosis during COVID-19. None of the remaining 3 ALL/LBL patients developed ARDS. None of the 4 ALL/LBL patients died. The patient with deep vein thrombosis did not receive further pegylated asparaginase.
Methods
Data of the clinical course were collected from the patient’s electronic medical records. Diagnosis of SARS-CoV-2 infection was based on virus detection by real-time polymerase chain reaction (SARS-CoV-2 E-gene RT-PCR) in respiratory tract specimens.3 SARS-CoV-2 immunoglobulin G (IgG) antibodies were tested against viral spike protein (S1/S2) and nucleoprotein (N).
Results and discussion
The median age of patients was 60 years (r, 32-76 years). Seventy-five percent (n = 9) were male. Four patients (33%) were asymptomatic at SARS-CoV-2 diagnosis, but later on, all patients became symptomatic. Ten patients (83%) were admitted to the intensive care unit (ICU). Eleven patients (92%) developed COVID-19 pneumonia. None of the 4 refractory AML patients developed ARDS. However, all 4 patients with newly diagnosed AL (patients 1, 2, 7, and 11) and the AML patient in CRi developed severe ARDS (median Pao2/Fio2 [Horovitz index] of 75 [r, 55-85])4 and septic shock. Overall, 5 patients were intubated (50%): 1 patient received high-flow oxygen and 1 ECMO therapy. Median duration between the beginning of symptoms and diagnosis of ARDS was 8 days (r, 4-20 days).
Deep vein thrombosis was observed in 1 patient despite adequate anticoagulation.5 The median stay at the ICU was 9 days (range, 2-23 days). Overall, 9 of 12 patients (75%) had aplasia (grade 4 neutropenia) during SARS-CoV-2 infection with a median duration of 33.5 days (r, 4-43 days). Six of 12 patients (50%) had grade 4 lymphopenia during clinical course (for laboratory values, see Table 2).
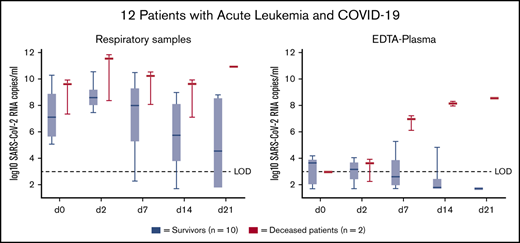
At diagnosis, SARS-CoV-2-RNA was detected in the upper respiratory tract samples of all patients (12 of 12) by RT-PCR at high concentrations (average 1 × 107 RNA copies per milliliter).3 All 10 tested patients showed viremia with an average of 1 × 103 RNA copies per milliliter at diagnosis. At day 14, viral loads in respiratory samples and blood decreased overall by 1 log. Four patients still showed viremia after 14 days. Only 7 of 10 tested patients (70%) developed reactivity in SARS-CoV-2 serology (IgM and IgG) after a median follow-up of 43 days (range, 12-61 days): 1 of these patients received COVID convalescent plasma. At the end of follow-up, 2 of 10 alive patients still had detectable SARS-CoV-2 RNA in nasopharyngeal swabs (20%).
All cases in which chest computed tomography (CT) scanning was performed showed bilateral, mainly peripheral, ground-glass opacities with (n = 4) or without (n = 2) consolidation, matching the typical finding of SARS-CoV-2 infection (according to Simpson et al and Li et al6,7 ). At time of CT scanning, 3 patients were in aplasia (patients 2, 6, and 9). Nevertheless, they were able to mount the typical infiltrates.
Three of 5 patients with ARDS were successfully extubated after invasive ventilation with a median time of 7 days (r, 4-12 days). Overall, 8 patients have been discharged from the ICU. Two patients have died (17%; patients 2 and 5). In contrast to the other patients, these patients showed no reduction in viral load in EDTA plasma at day 14 (see visual abstract).
In 7 cases, leukemia-specific treatment was adjusted. In 2 fit patients with newly diagnosed untreated AML (patients 7 and 11), the decision was made against intensive chemotherapy in favor of azacytidine/venetoclax. In all refractory patients (patients 6, 8, 9, and 10), the usual treatment plan was changed from intensive salvage chemotherapy to azacytidine/venetoclax. With this treatment strategy, comparable remission rates to those in non–SARS-CoV-2–infected patients could be observed.2 The patient with newly diagnosed B-ALL had to discontinue pegylated-asparaginase treatment due to COVID-19–associated deep vein thrombosis.
Clinical symptoms of COVID-19 range from mild symptoms to critical courses and even death.8 In unselected patients in China, mild and moderate courses have been described in ∼80%, almost 14% had severe disease, and 6% critical courses.8 We scored mild or moderate courses of COVID-19 in 3 patients (25%) and severe and critical courses in 9 patients (75%), including 2 deaths and 42% of severe ARDS. This corresponds to an almost 7 times higher rate of severe and critical courses of COVID-19 in patients with AL and LBL. In April 2020, He et al reported more severe SARS-CoV-2 infections in patients with hematological malignancies.9
The prolonged and severe course of clinical disease is paralleled by the virological findings showing that, during the long observation period in 2 patients, SARS-CoV-2 is still detectable and just 60% developed SARS-CoV-2 IgG/IgM. Remarkably, 4 of our patients had persistent viremia on day 14. Increasing RNA titers over the observation period were observed in the 2 patients who had a fatal outcome, which highlights the importance of monitoring RNA load in plasma.
The American Society of Hematology recommends treatment with intensive chemotherapy in patients with newly diagnosed AML and eligibility for intensive therapy.10 Although the number in our case series is small, only 1 of 4 patients with ALL/LBL developed a critical disease state. In all 4 patients, ALL-specific therapy could be administered with only small delays or modifications. All patients with newly diagnosed AML developed critical courses with ARDS, especially those treated with intensive chemotherapy. None of the 4 refractory AML patients who were all treated with azacytidine/venetoclax developed ARDS. This combination may be less toxic than intensive chemotherapy and may be used as a bridge to further therapy. Meanwhile, after full recovery from COVID-19, 6 patients with indication for stem cell transplantation could receive transplants without SARS-CoV-2 reactivation; another 2 patients are scheduled for transplantation.
To be able to draw firm conclusions on the treatment of AL from the pooled shared experience of the SARS-CoV-2–infected patients, international series are necessary.
Requests for data may be e-mailed to the corresponding author, Walter Fiedler, at fiedler@uke.de.
Authorship
Contribution: S.G., K.R., P.S., P.K., O.B., S.K., S.S., K.W., C.B., D.W., W.F., D.J., and F.M. collected the clinical and epidemiological data and summarized all data; S.P., H.R., and M.L. performed the virological and RT-PCR assays; H.I. was responsible for radiological assessment and analysis; S.G., S.P., K.R., D.W., W.F., D.J., and F.M. drafted the manuscript; S.G., C.B., D.W., W.F., and F.M. revised the final version; and all authors reviewed and approved the manuscript.
Conflict-of-interest disclosure: P.K. is a shareholder of Abbvie Inc. S.K. received research support by Ambu, E.T. View Ltd, Fisher & Paykel, Pfizer, and Xenios; received lecture honoraria from Arjo-Huntleigh, Astellas, Astra, Basilea, Bard, Baxter, Biotest, CSL Behring, Cytosorbents, Fresenius, Gilead, Merck Sharp & Dohme (MSD), Orion, Pfizer, Philips, Sedana, Sorin, Xenios, and Zoll; and received consultant honoraria from AMOMED, Astellas, Baxter, Bayer, Fresenius, Gilead, MSD, Pfizer, and Xenios. H.R. received speaker honoraria from MSD, Pfizer, Infectopharm, Correvio, Accelerate Diagnostics and as an advisor for MSD, Pfizer, and Shionogi. K.W. received speaker honoraria from Amgen, Adaptive, Bristol Myers Squibb (BMS), Celgene, Janssen, GlaxoSmithKline (GSK), Karyopharm, Takeda, and Sanofi; has participated in advisory boards/has a consulting role for Amgen, Adaptive, BMS, Celgene, Janssen, GSK, Karyopharm, Takeda, and Sanofi; and received research funding from Amgen, Celgene, Sanofi, and Janssen. C.B. received speaker honoraria from Merck KGaA, Sanofi, Roche, Bayer, BMS, AstraZeneca, and MSD; has a consulting or advisory role for Lilly/ImClone, Merck Serono, Sanofi, Bayer Schering Pharma, MSD, GSO, and AOK Health Insurance; received research funding from AbbVie, ADC Therapeutics, Agile Therapeutics, Alexion Pharmaceuticals, Amgen, Apellis Pharmaceuticals, Astellas Pharma, AstraZeneca, Bayer, BerGenBio, Blueprint, Medicines, BMS, Boehringer Ingelheim, Celgene, Daiichi Sankyo, Eisai, Gilead Sciences, Gylcotope GmbH, GSK, Incyte, IO Biotech, Isofol Medical, Janssen-Cilag, Karyopharm Therapeutics, Lilly, Millennium, MSD, Nektar, Novartis, Rafael Pharmaceuticals, Roche, Springworks Therapeutics, and Taiho Pharmaceutical; and received travel accommodations and expenses from Merck Serono, Sanofi, Pfizer, and BMS. D.W. reports personal fees from Correvio, Gilead, Pfizer, and MSD. W.F. has participated in advisory boards for Amgen, Pfizer, Novartis, Jazz Pharmaceuticals, Celgene, Morphosys, and Ariad/Incyte; received research funding from Amgen; received support for meeting attendance from Amgen, Jazz Pharmaceuticals, Daiichi Sankyo Oncology, and Servier; and has received support in medical writing from Amgen, Pfizer, and AbbVie. F.M. received support for meeting attendance from Servier, Incyte, Gilead, Jazz Pharmaceuticals, Novartis, Teva, Pfizer, and Amgen; received a research grant from Daiichi Sankyo; and received a speaker honorarium from Servier. The remaining authors declare no competing financial interests.
Correspondence: Walter Fiedler, II. Department of Internal Medicine, Oncology, Hematology and Bone Marrow Transplantation with Section Pneumology, University Cancer Center Hamburg, University Medical Center Hamburg-Eppendorf, N27, Ground Floor, Room 00.003.01, Martinistr 52, 20246 Hamburg, Germany; e-mail: fiedler@uke.de.