Key Points
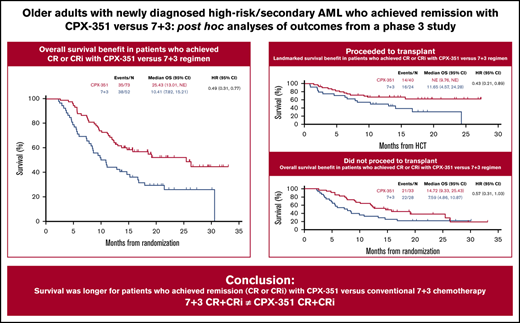
CPX-351 demonstrated longer median OS vs 7+3 among older adults with newly diagnosed high-risk/secondary AML who achieved remission.
The OS benefit was observed across the evaluated patient subgroups and irrespective of subsequent hematopoietic cell transplantation.

Abstract
CPX-351, a dual-drug liposomal encapsulation of daunorubicin/cytarabine in a synergistic 1:5 molar ratio, is approved for the treatment of adults with newly diagnosed, therapy-related acute myeloid leukemia (t-AML) or AML with myelodysplasia-related changes (AML-MRC). In a pivotal phase 3 study, patients aged 60 to 75 years with newly diagnosed, high-risk/secondary AML were randomized to receive CPX-351 or conventional 7+3 chemotherapy. In the primary endpoint analysis, CPX-351 demonstrated significantly prolonged median overall survival (OS) vs 7+3. These exploratory post hoc subgroup analyses evaluated the impact of achieving complete remission (CR) or CR with incomplete neutrophil or platelet recovery (CRi) with CPX-351 (73/153 [48%]) vs conventional 7+3 (52/56 [33%]) on outcomes. CPX-351 improved median OS vs 7+3 in patients who achieved CR or CRi (25.43 vs 10.41 months; hazard ratio = 0.49; 95% confidence interval, 0.31, 0.77). Improved median OS was seen across AML subtypes (t-AML, AML-MRC), age subgroups (60 to 69 vs 70 to 75 years), patients with prior hypomethylating agent exposure, and patients who did not undergo transplantation. Patients who achieved CR or CRi with CPX-351 also had a higher rate of transplantation, a longer median OS landmarked from the date of transplantation (not reached vs 11.65 months; hazard ratio = 0.43; 95% confidence interval, 0.21, 0.89), and a safety profile that was consistent with the known safety profile of 7+3. These results suggest deeper remissions may be achieved with CPX-351, leading to improved OS. This study was registered at www.clinicaltrials.gov as #NCT01696084.
Introduction
Secondary acute myeloid leukemia (sAML), which generally refers to the development of acute myeloid leukemia (AML) following a prior myeloid malignancy or as a late complication of chemotherapy or ionizing radiation (therapy-related acute myeloid leukemia [t-AML]),1,2 is historically associated with poorer outcomes with conventional induction chemotherapy when compared with other AML subtypes.3-10
CPX-351 (United States: Vyxeos, daunorubicin and cytarabine liposome for injection; Europe: Vyxeos Liposomal, liposomal daunorubicin and cytarabine powder for concentrate for solution for infusion) is a dual-drug liposomal encapsulation of daunorubicin and cytarabine approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of adults with newly diagnosed t-AML or AML with myelodysplasia-related changes (AML-MRC).11,12 CPX-351 was designed to improve efficacy vs conventional chemotherapy through the coencapsulation of daunorubicin and cytarabine at a synergistic 1:5 molar ratio within a bilayer liposome.13 Unlike conventional chemotherapy, the CPX-351 liposome is maintained in human plasma for up to 24 hours, with detectable drug present >7 days postadministration.14,15 The CPX-351 liposome also enables intracellular delivery of the synergistic drug ratio and enhances uptake in leukemia cells to a greater extent than normal cells in the bone marrow.16,17 In the primary analysis of data from the pivotal randomized phase 3 study in older adults with newly diagnosed high-risk/sAML, induction followed by consolidation with CPX-351 demonstrated a significantly improved median overall survival (OS [primary endpoint]; 9.56 vs 5.95 months; hazard ratio [HR] = 0.69; 95% confidence interval [CI], 0.52, 0.90; 1-sided P = .003) and a higher rate of complete remission (CR) or CR with incomplete neutrophil or platelet recovery (CRi) vs conventional 7+3 (48% vs 33%; 2-sided P = .016), with a safety profile that was consistent with the known safety profile of 7+3.18 After 5 years of follow-up, survival benefit was maintained.19
Unfortunately, remission achieved with conventional chemotherapy in sAML is less durable than in de novo AML. This was shown in a large registry study that found patients with either an antecedent hematologic disorder or t-AML who achieved CR with conventional chemotherapy had significantly shorter OS landmarked from the time of CR compared with de novo AML, irrespective of cytogenetic risk group.20 It is not known whether achievement of remission with newer agents, such as CPX-351, will translate into a similar benefit in outcomes as conventional chemotherapy or if the differences in the design and pharmacokinetic properties of CPX-351 may translate into deeper remissions and improved outcomes in those who achieve remission. Therefore, exploratory post hoc subgroup analyses of the CPX-351 pivotal phase 3 study were performed to explore the impact of achieving remission with CPX-351 vs conventional 7+3 on survival, hematopoietic cell transplantation (HCT), and safety outcomes in older adults with newly diagnosed high-risk/sAML.
Materials and methods
Study design
In this open-label, controlled, multicenter, phase 3 trial (ClinicalTrials.gov Identifier: #NCT01696084), patients were randomized 1:1 to receive induction therapy with CPX-351 or 7+3 chemotherapy, as described previously.18 Patients could receive up to 2 cycles of induction with CPX-351 100 units/m2 (daunorubicin 44 mg/m2 plus cytarabine 100 mg/m2) administered as a 90-minute infusion on days 1, 3, and 5 (days 1 and 3 for second induction) or with a 7+3 regimen consisting of cytarabine 100 mg/m2 per day continuous infusion for 7 days (5 days for second induction) plus daunorubicin 60 mg/m2 on days 1, 2, and 3 (days 1 and 2 for second induction). A second induction was highly recommended for any patient with documented reduction in leukemia burden and was mandatory for patients achieving >50% reduction in blast count at day 14. Patients who were not expected to receive second induction included those with evidence of aplasia/hypoplasia (<5% blast count) or equivocal bone marrow assessments.
Patients who achieved CR or CRi could receive up to 2 cycles of consolidation with CPX-351 65 units/m2 (daunorubicin 29 mg/m2 plus cytarabine 65 mg/m2) administered as a 90-minute infusion on days 1 and 3 or with the 5+2 regimen, consisting of cytarabine 100 mg/m2 per day continuous infusion for 5 days plus daunorubicin 60 mg/m2 on days 1 and 2. Patients could receive HCT at the discretion of the treating physician.
This study was conducted in accordance with the principles of the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice guidelines. The study protocol and all modifications were approved by the institutional review board or independent ethics committee at each study site, and all patients provided written informed consent prior to study participation.
Eligibility criteria
Study eligibility criteria have been described in detail elsewhere.18 Briefly, patients were aged 60 to 75 years with a pathological diagnosis of AML according to World Health Organization 2008 criteria (≥20% blasts in peripheral blood or bone marrow) and high-risk/sAML based on prior cytotoxic treatment, history of myelodysplastic syndrome (MDS; with or without prior hypomethylating agents [HMAs]) or chronic myelomonocytic leukemia (CMML), or de novo AML with myelodysplasia-related cytogenetic abnormalities. Key exclusion criteria included acute promyelocytic leukemia t(15;17) or other favorable cytogenetics at screening, prior induction therapy for AML (except hydroxyurea), active secondary malignancy or central nervous system leukemia, history of myeloproliferative neoplasms other than CMML, or AML-MRC with only morphologic evidence of multilineage dysplasia.
Endpoints and assessments
The primary study endpoint, OS, has been reported previously.18 Secondary efficacy endpoints included remission rate (CR, CR+CRi; assessed according to the Revised International Working Group Criteria for AML21 ) and remission duration. The proportion of patients who underwent HCT was also evaluated. Safety outcomes included adverse events and laboratory assessments.
Patients enrolled in the phase 3 study who achieved CR or CRi during the study were included in these exploratory post hoc subgroup analyses. Among patients who achieved CR or CRi, further exploratory analyses were performed for the subgroups of patients with t-AML, AML-MRC, and prior HMA exposure, as well as by age (60 to 69 vs 70 to 75 years) and among those who did not proceed to HCT.
Statistical analyses
The efficacy and safety exploratory post hoc analyses described herein were performed in the subset of patients who achieved CR or CRi during the study.
Statistical methodology has been described previously.18 Briefly, time-to-event endpoints were assessed using a stratified log-rank test to compare treatment groups. The Kaplan-Meier method was used to estimate the distribution of these endpoints over time. HRs and 95% CIs were estimated using a Cox proportional hazards regression model. Remission rates and other binary measures were compared using a Mantel-Haenszel test.
Results
Patients
A total of 309 patients were randomized to treatment with CPX-351 (n = 153) or 7+3 (n = 156). Of these patients, 73 (48%) achieved CR+CRi with CPX-351 and 52 (33%) achieved CR+CRi with 7+3 (odds ratio [OR] = 1.77; 95% CI, 1.11, 2.81) and were included in this analysis, including 57 (37%) vs 40 (26%) who achieved a CR (OR = 1.69; 95% CI, 1.03, 2.78; Table 1). Higher rates of CR+CRi were achieved with CPX-351 vs 7+3 among the subgroup of patients with t-AML (47% vs 36%) and also the subgroup with AML-MRC (48% vs 33%).
Among patients who received only 1 induction cycle, CR+CRi rates were 55% (58/105) with CPX-351 vs 34% (34/100) with 7+3, including CR rates of 45% (47/105) with CPX-351 vs 28% (28/100) with 7+3. On the other hand, for patients who received 2 induction cycles, CR+CRi rates were 31% (15/48) with CPX-351 vs 35% (18/51) with 7+3, including CR rates of 21% (10/48) with CPX-351 vs 24% (12/51) with 7+3. In a multivariate analysis, karyotype (favorable/intermediate vs unfavorable; OR = 3.95; 95% CI, 2.12, 7.37; nominal P < .001), white blood cell count (<20 × 103/µL vs ≥20 × 103/µL; OR = 3.48; 95% CI, 1.47, 8.22; nominal P = .005), and treatment arm (CPX-351 vs 7+3; OR = 1.85; 95% CI, 1.12, 3.08; nominal P = .017) were associated with achievement of CR or CRi. Furthermore, although karyotype, sex, white blood cell count, and treatment arm were associated with achievement of CR, only karyotype was associated with achievement of CRi (supplemental Table 1).
Baseline characteristics for all patients who achieved CR, CRi, and CR or CRi were generally balanced between CPX-351 and 7+3 treatment arms (Table 2). Although randomization into the study was stratified for sAML subtype, the treatment groups were not necessarily still balanced for sAML subtype among patients who achieved CR or CRi. Fewer patients with t-AML who achieved CR or CRi after CPX-351 vs 7+3 had received prior nonanthracycline chemotherapy alone (n = 2/14 [14%] vs n = 5/12 [42%]), whereas prior radiation therapy alone was less frequent in patients receiving 7+3 (n = 5/14 [36%] vs n = 2/12 [17%]). Among patients with AML-MRC who achieved CR or CRi, fewer patients receiving CPX-351 vs 7+3 had antecedent MDS with prior HMAs (n = 18/59 [31%] vs n = 18/40 [45%]), and more patients receiving CPX-351 had de novo AML with MDS karyotype (n = 23/59 [39%] vs n = 12/40 [30%]).
Duration of remission and relapse-free survival
For all patients with CR or CRi, the median duration of remission was 6.93 months with CPX-351 vs 6.11 months with 7+3 (HR = 0.77; 95% CI, 0.47, 1.26). Among patients who achieved CR, the median duration of remission was 7.89 vs 6.54 months (HR = 0.90; 95% CI, 0.54, 1.49), and among patients who achieved CRi, the median duration of remission was 5.32 vs 3.09 months (HR = 0.46; 95% CI, 0.17, 1.20).
Among patients who achieved CR, median relapse-free survival was also longer with CPX-351 vs 7+3 (11.24 vs 8.82 months; HR = 0.65; 95% CI, 0.39, 1.06).
OS
Median OS was longer with CPX-351 vs 7+3 in patients who achieved CR or CRi (25.43 vs 10.41 months; HR = 0.49; 95% CI, 0.31, 0.77; Figure 1A). Median OS was longer with CPX-351 vs 7+3 both in patients who achieved CR (25.43 months [n = 57] vs 10.97 months [n = 40]; HR = 0.49; 95% CI, 0.29, 0.83) and in those who achieved CRi (13.70 months [n = 16] vs 8.97 months [n = 12]; HR = 0.48; 95% CI, 0.19, 1.26). In a multivariate analysis, karyotype (favorable/intermediate vs unfavorable; HR = 0.48; 95% CI, 0.30, 0.79; nominal P = .003), platelet count (≤50 ×103/µL vs >50 × 103/µL; HR = 1.83; 95% CI, 1.11, 3.01; nominal P = .017), and treatment arm (CPX-351 vs 7+3; HR = 0.40; 95% CI, 0.25, 0.65; nominal P < .001) were associated with OS among patients who achieved CR or CRi (supplemental Table 2).
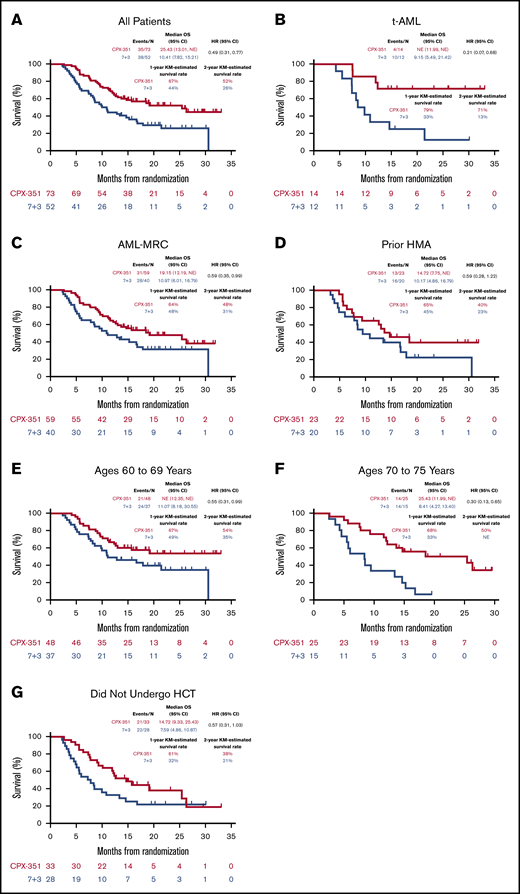
OS in patients who achieved CR or CRi. Among patients who achieved CR or CRi, median OS was numerically longer with CPX-351 vs 7+3 overall (A) and generally across the evaluated subgroups of patients (B-G). KM, Kaplan-Meier; NE, not estimable.
OS in patients who achieved CR or CRi. Among patients who achieved CR or CRi, median OS was numerically longer with CPX-351 vs 7+3 overall (A) and generally across the evaluated subgroups of patients (B-G). KM, Kaplan-Meier; NE, not estimable.
In addition, among patients who achieved CR or CRi, median OS was numerically longer with CPX-351 vs 7+3 overall (Figure 1A) and in subgroups of patients with t-AML, with AML-MRC, and ages 60 to 69 and 70 to 75 years (Figure 1B-F), with the most notable improvements in OS observed among patients with t-AML (not reached vs 9.15 months; HR = 0.21; 95% CI, 0.07, 0.68; Figure 1B) and those aged 70 to 75 years (25.43 vs 8.41 months; HR = 0.30; 95% CI, 0.13, 0.65; Figure 1F). However, it should be noted that the number of patients in some subgroups was small.
Among patients who achieved CR or CRi and did not undergo HCT (CPX-351: n = 33; 7+3: n = 28), median OS was numerically longer with CPX-351 vs 7+3 (14.72 vs 7.59 months; HR = 0.57; 95% CI, 0.31, 1.03; Figure 1G). Within this subgroup, median OS was 15.74 months with CPX-351 vs 7.36 months with 7+3 (HR = 0.53; 95% CI, 0.23, 1.22) among patients aged 60 to 69 years and was 12.19 months vs 8.41 months (HR = 0.47; 95% CI, 0.19, 1.21) among patients aged 70 to 75 years. Median OS was numerically longer with CPX-351 vs 7+3 both in patients who achieved CR and did not undergo HCT (19.15 months [n = 27] vs 8.41 months [n = 21]; HR = 0.55; 95% CI, 0.27, 1.10) and in those who achieved CRi and did not undergo HCT (8.54 months [n = 6] vs 5.13 months [n = 7]; HR = 0.61; 95% CI, 0.18, 2.03). Of note, the majority of patients who achieved CR or CRi but did not undergo HCT received postremission consolidation in both the CPX-351 (1 cycle: 8/33 [24%]; 2 cycles: 16/33 [48%]) and 7+3 (1 cycle: 13/28 [46%]; 2 cycles: 7/28 [25%]) treatment arms; for these patients, median OS was 13.67 months with CPX-351 vs 8.44 months with 7+3 (HR = 0.62; 95% CI, 0.31, 1.26). The remaining patients who achieved CR or CRi but did not receive consolidation or proceed to HCT discontinued treatment (CPX-351: n = 6; 7+3: n = 4), relapsed (CPX-351: n = 2; 7+3: n = 4), or did not receive further treatment per their physician’s choice (CPX-351: n = 1; 7+3: n = 0).
HCT outcomes
Fifty-two (34%) of 153 patients receiving CPX-351 and 39 (25%) of 156 patients receiving 7+3 underwent HCT in this study. Most patients who underwent HCT were in CR or CRi in both the CPX-351 arm (CR: 30/52 [58%]; CRi: 10/52 [19%]) and the 7+3 arm (19/39 [49%]; 5/39 [13%]).18 Among patients who achieved CR or CRi, the HCT rate was numerically higher with CPX-351 vs 7+3 (40/73 [55%] vs 24/52 [46%]; OR, 0.71; 95% CI, 0.35, 1.44). The HCT rate with CPX-351 vs 7+3 was 53% (30/57) vs 48% (19/40) in patients who achieved CR and 63% (10/16) vs 42% (5/12) in patients who achieved CRi. Among patients who achieved CR or CRi, the HCT rate was numerically higher with CPX-351 vs 7+3 in all evaluated subgroups except for patients with t-AML (supplemental Table 3). Postremission consolidation prior to HCT was common in both treatment arms: among patients who proceeded to HCT, 60% of patients in the CPX-351 arm received consolidation prior to their HCT (1 cycle: 17/40 [43%]; 2 cycles: 7/40 [18%]) compared with 50% in the 7+3 arm (1 cycle: 7/24 [29%]; 2 cycles: 5/24 [21%]).
Overall, median OS landmarked from the date of HCT was numerically longer with CPX-351 vs 7+3 in patients who achieved CR or CRi (not reached vs 11.65 months; HR = 0.43; 95% CI, 0.21, 0.89; Figure 2A). Median OS landmarked from the date of HCT with CPX-351 vs 7+3 was not reached vs 10.25 months in patients who achieved CR (HR = 0.43; 95% CI, 0.19, 0.96) and not reached vs 14.09 months in patients who achieved CRi (HR = 0.43; 95% CI, 0.09, 2.13). Median OS landmarked from the date of HCT was numerically longer with CPX-351 vs 7+3 in the evaluated subgroups of patients (Figure 2B-F), most notably those with t-AML (not reached vs 6.60 months; HR = 0.10; 95% CI, 0.01, 0.84; Figure 2B) and those aged 70 to 75 years (not reached vs 4.14 months; HR = 0.09; 95% CI, 0.02, 0.53; Figure 2F). However, it should be noted that the number of patients in some of the evaluated subgroups was small.
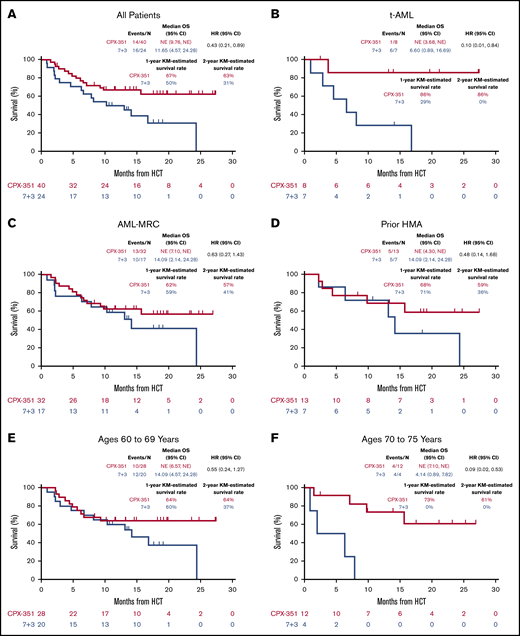
OS landmarked from the HCT date in patients who achieved CR or CRi. Among patients who achieved CR or CRi and subsequently underwent HCT, median OS landmarked from the HCT date was numerically longer with CPX-351 vs 7+3 overall (A) and across the evaluated subgroups of patients (B-F).
OS landmarked from the HCT date in patients who achieved CR or CRi. Among patients who achieved CR or CRi and subsequently underwent HCT, median OS landmarked from the HCT date was numerically longer with CPX-351 vs 7+3 overall (A) and across the evaluated subgroups of patients (B-F).
Safety and tolerability
The safety profile of CPX-351 in patients who achieved CR or CRi was generally consistent with the overall study population and the known safety profile of 7+3 (Table 3). In patients who achieved CR or CRi, the most frequently reported grade 3 to 5 treatment-emergent adverse events (TEAEs; ≥10% of patients) at any time during the study were febrile neutropenia (CPX-351: 79% vs 7+3: 77%), hypertension (14% vs 6%), pneumonia (12% vs 15%), bacteremia (11% vs 2%), sepsis (6% vs 10%), and pulmonary edema (3% vs 10%). Febrile neutropenia (CPX-351: 15% vs 7+3: 12%) was the most frequently reported serious TEAE. Only 1 patient experienced discontinuation because of a TEAE in the CPX-351 arm (cardiac failure).
Four patients who achieved CR or CRi died during the postremission phase because of the following causes: sepsis (CPX-351), atrial fibrillation (7+3), disease progression (7+3), and intracranial hemorrhage (7+3). No patient experienced early mortality (within 60 days of treatment initiation) in either treatment arm.
CPX-351 was associated with a longer median time to recovery of neutrophils and platelets vs 7+3 in all patients who achieved CR or CRi (Table 4). Similar results were observed for the subgroups of patients with t-AML, AML-MRC, and prior HMA exposure, as well as by age subgroups.
Discussion
CPX-351 is a dual-drug liposomal encapsulation of daunorubicin and cytarabine at a synergistic 1:5 molar ratio14 that has shown significantly improved survival, higher remission rates, and comparable safety to that of the conventional 7+3 regimen in older patients with high-risk/sAML in a large, multicenter, randomized, controlled, phase 3 trial.18 Consistent with these findings, results from these exploratory post hoc subgroup analyses demonstrated that, among the overall group of patients who achieved remission, CPX-351 improved median OS and the likelihood of proceeding to HCT vs 7+3, suggesting the potential for achievement of deeper responses with CPX-351, although this hypothesis needs to be confirmed in a subsequent study. Furthermore, median OS was numerically longer with CPX-351 vs 7+3 in subgroups of patients with t-AML and AML-MRC, as well as by age subgroups and among patients who did not undergo HCT, although the most notable improvements in OS were observed for those with t-AML and among older patients (aged 70 to 75 years). However, the ability to form definitive conclusions based on these data is limited by the small number of patients in some subgroups.
The assessment of measurable residual disease (MRD) in patients with AML who achieve remission provides powerful prognostic information. Unfortunately, the assessment of MRD was not prospectively collected in this study, and there are insufficient banked patient samples to assess MRD. Although MRD results are not available from this phase 3 study, the hypothesis of deeper remissions achieved with CPX-351 vs 7+3 is suggested by studies of real-world evidence with CPX-351 that have reported notable proportions of responders achieving MRD negativity. A compassionate use program from 33 centers in Italy evaluated the clinical activity of CPX-351 in patients with t-AML or AML-MRC in a real-life setting. Results from this study indicated a CR+CRi rate of 65% in 71 evaluable patients after cycle 1, with 70% achieving CR by the end of treatment. MRD was assessed with multicolor flow cytometry (negativity defined as <0.01%) and/or Wilms tumor (WT1) gene expression levels. Following the first induction, multicolor flow cytometry MRD negativity was achieved in 15/40 (38%) assessed patients, whereas WT1 MRD negativity was achieved in 21/38 (55%) assessed patients.22 A multicenter, retrospective study evaluated the efficacy of CPX-351 in patients with newly diagnosed t-AML or AML-MRC from 12 centers in France. CR+CRi was achieved by 61/103 (59%) patients, including 57 (55%) with CR. MRD negativity at the 10−3 sensitivity threshold (assessed with flow cytometry, next-generation sequencing, or real-time quantitative polymerase chain reaction) was achieved in 16/28 (57%) responders with an MRD evaluation at the first consolidation cycle.23 In another multicenter, retrospective study that evaluated the efficacy of CPX-351 in patients who primarily had t-AML or AML-MRC, CR+CRi was achieved by 41/66 (62%) patients with wild-type TP53, including 30 (45%) with CR. Among patients with wild-type TP53 who achieved CR, MRD negativity was reported for 9/25 (36%) patients with an MRD evaluation.24 However, it should be noted that these studies were not designed to compare outcomes observed for CPX-351 with conventional chemotherapy, and it will be important to include MRD assessments in future clinical studies of CPX-351.
The achievement of deep remissions with CPX-351 is important, as historically remission alone did not necessarily translate into a survival benefit, and survival rates remain low among sAML patients who achieve remission with conventional chemotherapy.20 Results of the current study demonstrated that, compared with conventional 7+3 chemotherapy, CPX-351 not only improves remission rates in patients with high-risk/sAML but also survival outcomes among those who achieved CR or CRi. Key differences between the CPX-351 liposome and conventional 7+3 chemotherapy include the prolonged and coordinated pharmacokinetics of daunorubicin and cytarabine with the CPX-351 liposome14 and persistent drug exposure at a synergistic ratio within the bone marrow.13 Furthermore, the CPX-351 liposome enables intracellular delivery with greater uptake in leukemic cells than normal cells in the bone marrow.16,17
Allogeneic HCT is recommended as postremission therapy in order to prolong remission and prevent recurrence in patients with AML25 ; it is currently the most effective therapy with curative intent for patients with intermediate- or poor-risk AML. Patients who achieved CR or CRi with CPX-351 in this study were more likely to proceed to HCT and had a longer median OS landmarked from the date of HCT vs those who achieved remission with 7+3 chemotherapy, suggesting CPX-351 is a viable option for patients in whom HCT can be considered. Similar to findings for median OS, this improvement in median OS landmarked from the date of HCT vs 7+3 was most notable for patients with t-AML, and among older patients (aged 70 to 75 years) who achieved CR or CRi, and the number of patients in some subgroups was small. We cannot be certain whether the difference in number of second consolidation cycles prior to HCT contributed to the more favorable post-HCT survival observed with CPX-351, although this remains a possibility.
It is also noteworthy that median OS was also longer with CPX-351 vs 7+3 among patients who achieved CR or CRi but did not subsequently undergo HCT, suggesting a treatment benefit of remission with CPX-351 even among patients who do not proceed to HCT.
The CPX-351 safety profile in these subgroups was consistent with the overall study population18 and known safety profile of 7+3. Of note, as expected and observed in the overall study population,18 median time to recovery of neutrophils and platelets was longer with CPX-351 vs 7+3 in all subgroups of patients; the prolonged myelosuppression observed with CPX-351 may be attributed to the prolonged drug exposure observed with CPX-351.14,15 Importantly, despite prolonged myelosuppression, no patient experienced early mortality (within 60 days of treatment initiation) in the CPX-351 arm.
In summary, CPX-351 has demonstrated longer median OS, a higher rate of patients undergoing HCT, longer median OS landmarked from the date of HCT, and comparable safety to that of conventional 7+3 chemotherapy among patients who achieved CR or CRi in this population of older adults with newly diagnosed high-risk/sAML. Although it was not possible to evaluate the depth of remission via MRD assessments, results of the current analyses suggest the remissions achieved with CPX-351 treatment may permit more patients to proceed to HCT and lead to prolonged survival; however, this observation needs to be confirmed in a subsequent study. Together, the findings from these subgroup analyses build upon and further strengthen the improved outcomes observed with CPX-351 vs 7+3 in the overall study population.
Relevant data are provided within this manuscript and supporting files, or within the files for the primary study publication by Lancet et al.18 For data sharing, please contact the corresponding author at tlin@kumc.edu.
Acknowledgments
The authors thank all of the patients who participated in the study and their families, as well as the investigators, nurses, coordinators, and other research staff at each study site. Medical writing and editorial support were provided by Senem Kurtoglu Lubin, of SciFluent Communications, Inc, under the direction of the authors and were financially supported by Jazz Pharmaceuticals.
This study was supported by Jazz Pharmaceuticals.
Authorship
Contribution: S.F. conceived and designed the study; T.L.L., D.A.R., D.H.R., G.J.S., J.E.K., G.L.U., D.E.H., S.R.S., M.J.W., J.E.C., and J.E.L. provided study materials or patients; T.L.L., D.A.R., D.H.R., G.J.S., J.E.K., G.L.U., D.E.H., S.R.S., M.J.W., J.E.C., and J.E.L. collected and assembled data; and all authors analyzed and interpreted the data; wrote the manuscript; and provided final approval of the manuscript.
Conflict-of-interest disclosure: D.A.R. served as a consultant for AbbVie, Novartis, Pfizer, Spectrum, and Teva; and served on speakers bureaus for Gilead, Incyte, Jazz Pharmaceuticals, Millennium, and Seattle Genetics. D.H.R. holds stock ownership in AbbVie and patents/royalties with the University of Rochester. G.J.S. received research funding from AbbVie, Agios, Actinium, Amgen, Ariad, Astellas Pharma, Bristol Myers Squibb, Constellation, Cyclacel, Daiichi Sankyo, Deciphera, Delta-Fly, Forma, Fujifilm, Gamida, Genentech-Roche, Geron, Incyte, Jazz Pharmaceuticals, Karyopharm, Kite Pharma, Mateon, MedImmune, Novartis, Onconova, Pfizer, REGiMMUNE, Samus, Sangamo, Tolero, and Trovagene; served as a consultant for Agios, Amgen, AstraZeneca, Incyte, Novartis, and Ono Pharma; served on speakers bureaus for Agios, Amgen, Celgene, Gilead, Incyte, Sanofi, and Stemline; provided expert testimony for Kaiser Permanente; and holds stock in Amgen, Bristol Myers Squibb, Johnson & Johnson, and Pfizer. J.E.K. received honoraria from Gilead, Magellan, and Novartis; served as a consultant for Gilead, Magellan, Novartis, Pharmacyclics, and Seattle Genetics; received research funding from Boehringer Ingelheim, Cantex, Erytech, and Millennium; and received travel support from Gilead, Novartis, and Seattle Genetics. G.L.U. served as a consultant for Jazz Pharmaceuticals and Genentech and received honoraria from Astellas Pharma. M.J.W. received research funding from Amgen, Leadiant, Merck, and Shire; participated in advisory committees for Daiichi Sankyo; and holds stock ownership in Reata Pharmaceuticals. R.J.R. and S.F. are employees of and hold stock ownership/options in Jazz Pharmaceuticals. J.E.C. served as a consultant for Astellas Pharma, Daiichi Sankyo, Jazz Pharmaceuticals, Novartis, and Pfizer; and received research funding from Arog, Astellas Pharma, Daiichi Sankyo, Jazz Pharmaceuticals, Novartis, and Pfizer. J.E.L. served as a consultant for Agios, Daiichi Sankyo, Jazz Pharmaceuticals, and Pfizer. The remaining authors declare no competing financial interests.
Correspondence: Tara L. Lin, University of Kansas Medical Center, 3901 Rainbow Blvd, Kansas City, KS 66103; e-mail: tlin@kumc.edu.