Key Points
Patients with relapsed or refractory NLPHL have a favorable overall prognosis.
Treatment of relapsed or refractory NLPHL should be chosen individually.

Abstract
The optimal treatment of patients with relapsed or refractory nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is ill defined. To shed more light on treatment options and outcome, we performed an analysis using the database of the German Hodgkin Study Group (GHSG). Ninety-nine patients who had received first-line treatment within 12 prospective GHSG studies conducted between 1993 and 2009, and subsequently developed disease recurrence (n = 91) or had primary disease progression (n = 8), were included. At initial NLPHL diagnosis, the median age was 40 years and 76% of patients were male. First-line treatment consisted of radiotherapy (RT) alone (20%), chemotherapy with or without RT (74%), and the anti-CD20 antibody (Ab) rituximab (6%), respectively. The median follow-up from initial diagnosis was 11.2 years. The median time to disease recurrence was 3.7 years. The applied salvage approaches included single-agent anti-CD20 Ab treatment or RT alone (37%), conventional chemotherapy (CT) with or without anti-CD20 Ab treatment with or without RT (27%) and high-dose chemotherapy (HDCT) followed by autologous stem cell transplantation (ASCT) (31%). No salvage treatment was given in 4% of patients. The 5-year progression-free survival and overall survival estimates after NLPHL recurrence were 75.6% and 89.5% (74.1% and 97.2% after single-agent anti-CD20 Ab treatment or RT alone; 68.0% and 77.8% after CT with or without anti-CD20 Ab treatment with or without RT; 84.6% and 89.8% after HDCT and ASCT). Hence, patients with relapsed or refractory NLPHL had a good overall prognosis. Factors such as time to disease recurrence and previous treatment may guide the choice of the optimal salvage approach for the individual patient.
Introduction
Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is a rare malignancy accounting for ∼5% of all Hodgkin lymphoma (HL) cases. The disease has distinct pathological and clinical characteristics. In contrast to classical HL (cHL), the malignant cells in NLPHL consistently express CD20 but are negative for CD30. The clinical course of NLPHL is usually rather indolent and most patients are diagnosed in early stages. However, especially late relapses occur more frequently than in cHL.1
The optimal treatment of relapsed or refractory NLPHL is ill defined. Several retrospective analyses have evaluated high-dose chemotherapy (HDCT) and autologous stem cell transplantation (ASCT). Results were at least comparable to those observed in relapsed cHL.2-4 However, aggressive salvage therapy may only be necessary in a minority of patients with NLPHL recurrence whereas most patients are likely treated sufficiently with less toxic approaches. Single-agent treatment with the anti-CD20 antibodies (Abs) rituximab and ofatumumab has been evaluated in prospective phase 2 studies. Response rates were close to 100% and long-term disease control was achieved in a relevant proportion of patients.5-7 Conventional chemotherapy (CT) and/or radiotherapy (RT) may also be considered but data on these approaches are scarce.8,9
To shed more light on treatment and clinical course of patients with relapsed or refractory NLPHL, we performed an analysis using the database of the German Hodgkin Study Group (GHSG). In addition to outcome parameters, we evaluated whether specific patient characteristics may have had influence on the applied second-line treatment. We also investigated the cause of death in those patients who had died during follow-up. Previous reports had indicated that NLPHL patients more often succumb to treatment-related late effects than the underlying lymphoma.10,11
Patients and methods
Patients and treatment
We screened the GHSG database for patients of all stages (early stages: stage I/II without risk factors; intermediate stages: stage I and IIA with at least 1 of the risk factors [a] elevated erythrocyte sedimentation rate defined as ≥50 mm/h in patients without B symptoms and ≥30 mm/h in patients with B symptoms, [b] involvement of ≥3 nodal areas, [c] extranodal disease and [d] large mediastinal mass greater than or equal to one-third of the maximum horizontal chest diameter; stage IIB with 1 or both of the risk factors [a] and [b]; advanced stages: stage IIB with 1 or both of the risk factors [c] and [d], stage III/IV) who had first-line treatment of newly diagnosed NLPHL (as confirmed by expert review) within 12 prospective GHSG trials (HD7-HD15, LP, LPHD, RIPL) conducted between 1993 and 2009.12-22 All studies were approved by the review boards of the participating sites and conducted in accordance with the Declaration of Helsinki. First-line treatment consisted of RT alone, chemotherapy with or without RT, and single-agent treatment with the anti-CD20 antibody (Ab) rituximab, respectively.
Patients with NLPHL recurrence during follow-up or primary disease progression (defined as disease progression during treatment or within the first 6 months after the end of treatment) were eligible for the present analysis. Lymphoma recurrence with histological transformation into aggressive B-cell non-Hodgkin lymphoma (B-NHL) was an exclusion criterion.
Follow-up
Follow-up was carried out regularly at the participating sites. Within the HD7-HD9 studies, follow-up visits took place every 3 months for the first 2 years, every 4 months until the end of the fourth year, and twice a year thereafter. Within the HD10-15, LP, LPHD, and RIPL studies, follow-up visits were conducted every 3 months within the first 6 (HD13-HD15), 12 (RIPL), or 24 (HD10-HD12, LP, LPHD) months, every 6 months until the end of the fourth year, and once a year thereafter. Within all studies, computed tomography scans during follow-up were only recommended in the case of suspicious clinical symptoms. In case NLPHL recurrence or primary disease progression were diagnosed, the date of diagnosis and the applied salvage treatment that was given at the discretion of the local investigator were recorded and reported to the trial coordination center of the GHSG.
Statistical methods
Descriptive statistics were used to summarize data. Median observation time (MOT) was defined as duration of follow-up after the initial NLPHL diagnosis. MOT after first relapse (MOT-2) was defined as duration of follow-up after the diagnosis of the first relapse or primary disease progression. Progression-free survival (PFS) after first relapse or primary disease progression (PFS-2) was defined as time from the diagnosis of the first relapse or primary disease progression until the occurrence of a second relapse or death from any cause and was censored for patients alive without second relapse at the date of the last documented follow-up visit. Overall survival (OS) after first relapse or primary disease progression (OS-2) was defined as time from the diagnosis of the first relapse or primary disease progression until death from any cause and was censored at the date of the last documented follow-up visit for surviving patients. MOTs as well as PFS-2 and OS-2 rates and 95% confidence intervals (CIs) were estimated using the Kaplan-Meier method. Statistical analyses were performed using SAS version 9.4.
Results
Patient characteristics
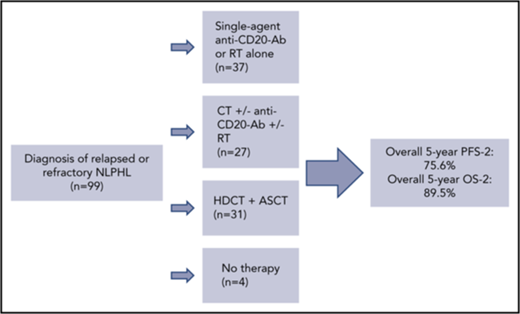
Within the 12 prospective GHSG studies taken into account, a total of 710 patients were treated for newly diagnosed NLPHL. Among those, 107 patients (15.1%) had disease recurrence (n = 99; 14.0%) or primary disease progression (n = 8; 1.1%). However, 8 patients with documented relapse but missing information on the applied salvage therapy were excluded so that 99 patients (91 with disease recurrence, 8 with primary disease progression) were ultimately included in the analysis.
The median age at the initial NLPHL diagnosis was 40 years (range, 16-75); 75 of 99 patients (76%) were male. Sixty-one of 99 patients (62%) initially presented with early stages, of whom 20 (33%), 35 (57%), and 6 (10%) had first-line treatment with RT alone, chemotherapy with or without RT, and the anti-CD20 Ab rituximab, respectively. Fourteen of 99 patients (14%) presented with intermediate stages and 24 of 99 patients (24%) with advanced stages. These patients all had chemotherapy with or without RT as first-line treatment. The MOT from the initial NLPHL diagnosis was 11.2 years for the whole patient group (Table 1).
The median time to first relapse was 3.7 years (range, 0.2-19.4). The median age at first relapse was 45 years (range, 20-79). The relapse occurred >5 years after the initial NLPHL diagnosis in 39 of 99 patients (39%) (data not shown).
Treatment at relapse or primary disease progression
Second-line treatment consisted of single-agent anti-CD20 Ab treatment or RT alone in 37 of 99 patients (37%), CT with or without anti-CD20 Ab treatment with or without RT in 27 of 99 patients (27%), and HDCT followed by ASCT in 31 of 99 patients (31%). Four of 99 patients (4%) did not receive any salvage therapy (Table 1).
Patients who had initially been diagnosed with early-stage disease received salvage therapy with single-agent anti-CD20 Ab treatment or RT alone in 25 of 61 cases (41%), CT with or without anti-CD20 Ab treatment with or without RT in 21 of 61 cases (34%), and HDCT followed by ASCT in 13 of 61 cases (21%). In patients with intermediate and advanced stages at initial diagnosis, salvage therapy consisted of single-agent anti-CD20 Ab treatment or RT alone in 4 of 14 patients (29%) and 8 of 24 patients (33%), CT with or without anti-CD20 Ab treatment with or without RT in 2 of 14 patients (14%) and 4 of 24 patients (17%), and HDCT followed by ASCT in 6 of 14 patients (43%) and 12 of 24 patients (50%) (Table 1).
Salvage therapy of patients who had received RT alone at initial diagnosis consisted of single-agent anti-CD20 Ab treatment or RT alone in 6 of 20 cases (30%), CT with or without anti-CD20 Ab treatment with or without RT in 13 of 20 cases (65%), and HDCT followed by ASCT in 1 of 20 cases (5%). Salvage therapy after chemotherapy with or without RT as first-line treatment consisted of single-agent anti-CD20 Ab treatment or RT alone in 26 of 73 cases (36%), CT with or without anti-CD20 Ab treatment with or without RT in 13 of 73 cases (18%), and HDCT and ASCT in 30 of 73 cases (41%). No second-line treatment was applied in 4 of 73 cases (5%). Patients who had initially received anti-CD20 Ab treatment with rituximab had second-line treatment with single-agent anti-CD20 Ab treatment or RT alone in 5 of 6 cases (83%) and CT with or without anti-CD20 Ab treatment with or without RT in 1 of 6 cases (17%). None of the patients initially treated with rituximab had HDCT and ASCT as salvage therapy (Table 2).
Second-line treatment consisted of HDCT and ASCT in 29 of 82 patients (35%) who were aged 60 years or younger at NLPHL recurrence. In contrast, this approach was applied in only 2 of 17 patients (17%) aged older than 60 years at the time of relapse or primary disease progression (data not shown). With respect to the time interval between initial NLPHL diagnosis and disease recurrence, 30 of 39 patients (77%) who had relapsed >5 years after the initial diagnosis were treated with single-agent anti-CD20 Ab treatment or RT alone or CT with or without anti-CD20 Ab treatment with or without RT as compared with 34 of 60 patients (57%) who had relapsed earlier. In contrast, only 8 of 39 patients (21%) with disease recurrence >5 years after the initial NLPHL diagnosis had HDCT and ASCT as salvage modality, whereas 23 of 60 patients (38%) with earlier recurrence of NLPHL were treated with this approach (data not shown).
PFS-2, subsequent relapses, and transformations
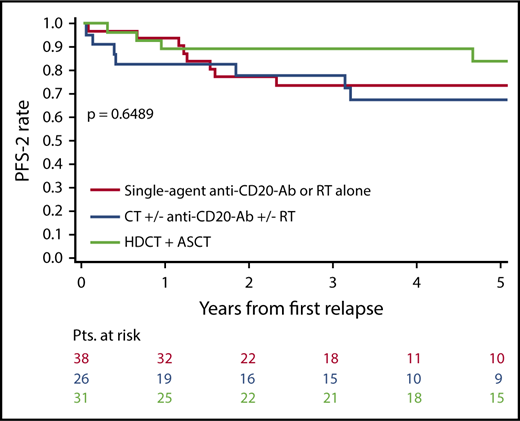
With an MOT-2 of 4.6 years, the 3-year and 5-year PFS-2 estimates for all 99 patients were 80.9% (95% CI, 72.5-89.4) and 75.6% (95% CI, 65.7-85.5), respectively (Table 3). There were no significant PFS-2 differences between the applied second-line approaches with 5-year PFS-2 estimates of 74.1% (95% CI, 58.5-89.7), 68.0% (95% CI, 48.1-87.9), and 84.6% (95% CI, 70.2-98.9) after single-agent anti-CD20 Ab treatment or RT alone, CT with or without anti-CD20 Ab treatment with or without RT, and HDCT and ASCT, respectively (P = .6489) (Figure 1; Table 3).
A second relapse was reported for 14 patients. Among those, 3 patients, 8 patients, and 3 patients had received second-line treatment with single-agent anti-CD20 Ab treatment or RT alone (MOT-2 = 3.8 years), CT with or without anti-CD20 Ab treatment with or without RT (MOT-2 = 4.6 years), and HDCT and ASCT (MOT-2 = 6.7 years), respectively (Table 3). Third-line treatment consisted of single-agent anti-CD20 Ab treatment or RT alone in 6 of 14 patients (43%), 3 of 14 patients (21%) had CT with or without anti-CD20 Ab treatment with or without RT, and HDCT and ASCT was applied in 2 of 14 patients (14%). No information on the third-line treatment was available for 3 of 14 patients (21%) (data not shown).
A third relapse occurred in 3 patients (Table 3). These patients had fourth-line treatment with single-agent anti-CD20 Ab treatment or RT alone (n = 1) and HDCT followed by ASCT (n = 2), respectively (data not shown).
None of the patients included in the present analysis developed histological transformation into aggressive B-NHL during follow-up.
OS-2 and causes of death
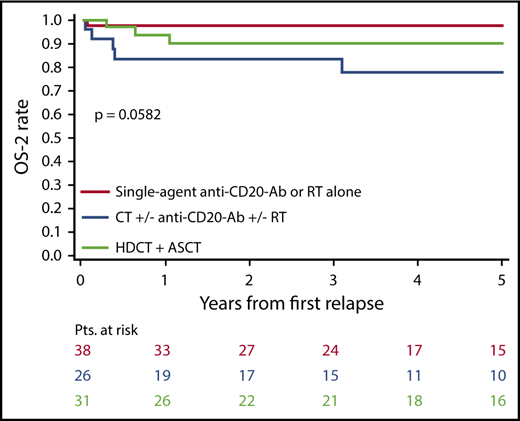
The 5-year OS-2 estimate for the whole patient group was 89.5% (95% CI, 82.9-96.1). Rates for the applied salvage approaches ranged between 77.8% with CT with or without anti-CD20 Ab treatment with or without RT and 97.2% with single-agent anti-CD20 Ab treatment or RT alone (P = .0582 for the comparison between single-agent anti-CD20 Ab treatment or RT alone, CT with or without anti-CD20 Ab treatment with or without RT, and HDCT and ASCT; P = .0148 for the comparison between single-agent anti-CD20 Ab treatment or RT alone and CT with or without anti-CD20 Ab treatment with or without RT) (Table 3; Figure 2) (data not shown).
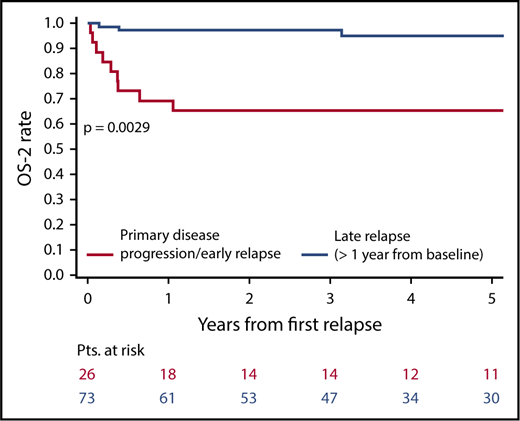
With 5-year OS-2 estimates of 65.4% (95% CI, 47.1-83.7) and 94.9% (95% CI, 89.1-100), respectively, survival for patients with primary disease progression or relapse within 1 year after the initial NLPHL diagnosis (n = 26) was significantly worse in comparison with those (n = 73) with later NLPHL recurrence (P = .0029) (Figure 3).
A total of 15 deaths occurred during follow-up. The underlying lymphoma was the cause of death in 9 cases (5 of 91 patients with relapsed NLPHL and 4 of 8 patients with primary disease progression), 3 patients died of second malignancies, and 3 patients from infectious complications (Table 2).
Discussion
To our knowledge, this is the largest analysis on characteristics, treatment, and outcome of patients with relapsed or refractory NLPHL. Overall, 99 patients were included. The major findings were as follows: (1) with an MOT-2 of 4.6 years, the 5-year OS-2 estimate for the whole patient group was close to 90%; (2) many patients do not appear to require HDCT and ASCT as salvage therapy but are treated sufficiently with less intensive approaches; and (3) early relapse and primary disease progression are associated with a dismal outcome and novel treatment approaches are needed for this patient group.
The patients included in the present analysis had their initial NLPHL diagnosis at a median age of 40 years and 76% of them were male. This is in line with previous reports. A larger analysis from the GHSG comprising 394 patients with newly diagnosed NLPHL who had received first-line treatment within prospective studies reported a median age of 37 years at initial diagnosis. The proportion of male patients was 76%.23 A population-based analysis using the Surveillance, Epidemiology, and End Results database identified 1162 patients who were diagnosed with NLPHL between 1988 and 2010. The median age at diagnosis was 38 years and 69% of patients were male.24
With an MOT of 11.2 years from the initial NLPHL diagnosis, 74% of patients with NLPHL recurrence had relapsed >1 year after the first NLPHL diagnosis. Disease recurrence occurred >5 years after the initial NLPHL diagnosis in 39% of patients. The median time interval between the initial NLPHL diagnosis and disease recurrence was 3.7 years. This finding is consistent with other analyses also showing a high rate of late relapses but only few cases of early disease recurrence and primary disease progression in NLPHL.23,25
Salvage therapy among the patients included in the present analysis consisted of single-agent anti-CD20 Ab treatment or RT alone in 37 of 99 patients (37%), CT with or without anti-CD20 Ab treatment with or without RT in 27 of 99 patients (27%), and HDCT followed by ASCT in 31 of 99 patients (31%). Different factors including the time interval between the initial NLPHL diagnosis and the occurrence of relapse, stage, and treatment at initial diagnosis and the age at relapse or primary disease progression appeared to have influence on the choice of the salvage strategy. Hence, only a small proportion of patients with a late relapse after nonaggressive first-line treatment had HDCT and ASCT at disease recurrence. These patients were more often treated with single-agent anti-CD20 Ab treatment or RT alone and CT with or without anti-CD20 Ab treatment with or without RT, respectively. In contrast, patients who had relapsed early after multiagent chemotherapy for advanced NLPHL had HDCT and ASCT as second-line approach in the majority of cases.
No PFS-2 differences were observed between the applied salvage strategies. However, the 5-year OS-2 estimate for patients treated with CT with or without anti-CD20 Ab with or without RT was significantly worse than for those receiving single-agent anti-CD20 Ab treatment or RT alone. This finding is likely due to a rather indolent course of disease in patients receiving salvage therapy with single-agent anti-CD20 Ab treatment or RT alone allowing a successful remission induction also in case subsequent relapses occur after second-line treatment. Conversely, some patients treated with CT with or without anti-CD20 Ab treatment with or without RT may have been candidates for more aggressive salvage therapy, for example, HDCT and ASCT.
Given the mostly indolent course of NLPHL, many patients with disease recurrence do not require intensive second-line treatment. Thus, some prospective phase 2 studies have investigated single-agent anti-CD20 Ab treatment in relapsed NLPHL. A phase 2 study from the GHSG evaluated the anti-CD20 Ab rituximab at a dose of 375 mg/m2 once weekly for 4 consecutive weeks in 15 patients with NLPHL recurrence. The overall response rate (ORR) was 94%. After a median follow-up of 63 months, the median time to progression was 33 months. Only 1 patient had died during observation.5 Another phase 2 study conducted in the United States also investigated single-agent rituximab. The Ab was given at a dose of 375 mg/m2 once weekly for 4 consecutive weeks either followed by rituximab maintenance every 6 months for 2 years or without subsequent treatment. A total of 18 patients with relapsed NLPHL were included. The ORR was 100%. After a median follow-up of 9.8 years, the 5-year PFS and OS rates for the 11 patients receiving 4 weekly rituximab doses only were 36.4% and 90.9%, respectively. The 5-year PFS and OS rates for the 7 patients treated with 4 weekly rituximab doses followed by rituximab maintenance were 71.4% each. The median follow-up of these patients was 4.2 years.6 More recently, a phase 2 study evaluating the second-generation anti-CD20 Ab ofatumumab in relapsed NLPHL revealed an ORR of 96%. After a MOT of 26 months, the 2-year PFS and OS rates were 80% and 100%.7 Taken together, single-agent anti-CD20 Ab treatment results in response rates close to 100% and induces long-term remissions in a relevant proportion of patients with relapsed NLPHL.
However, patients presenting with poor-risk features are candidates for aggressive salvage therapy with HDCT and ASCT. This approach has been evaluated in some retrospective analyses comprising patients with relapsed NLPHL. The largest analysis was performed by the European Group for Blood and Marrow Transplantation. A total of 60 patients who had received a median of 2 lines of treatment prior to HDCT and ASCT were included. The median time from NLPHL diagnosis to HDCT and ASCT was only 21 months. After a median follow-up of 56 months, the 5-year PFS and OS rates were 66% and 87%.2 Similar rates were obtained from several smaller analyses also addressing this issue.3,4
Data on the use of CT with or without anti-CD20 Ab treatment with or without RT in relapsed NLPHL are scarce. A retrospective study included 22 children who had NLPHL recurrence after initial treatment with resection alone, chemotherapy alone, or chemotherapy followed by consolidating RT. The majority had salvage treatment with CT. After a median follow-up of 21 months, 4 children had developed a second relapse. None of them had died.8 Another retrospective analysis including patients with newly diagnosed NLPHL demonstrated promising results with the combination of rituximab and CT according to the cyclophosphamide, doxorubicin, vincristine, prednisone (CHOP) protocol.26 This approach also represents a treatment option in some patients with relapsed NLPHL. However, additional studies addressing this issue are needed for final conclusions.
A total of 15 deaths occurred among the 99 NLPHL patients included in the present analysis. The cause of death was the underlying lymphoma in 9 cases (5 of 91 patients with relapsed disease and 4 of 8 patients with primary disease progression) whereas 6 deaths comprising 3 cases of second malignancies were possibly treatment-related. The latter finding underscores the need to optimize the risk-benefit ratio for both first-line treatment and salvage therapy by reducing the treatment burden whenever possible. However, patients with early relapse and primary disease progression have a dismal outcome. Therefore, novel combinations of aggressive chemotherapy and targeted drugs are required for this patient group.
Limitations of the present analysis include the small size of the treatment groups, the lack of expert review for a relevant proportion of biopsies obtained at disease recurrence, and the missing information on the stage at relapse for many patients taken into account. Nonetheless, the analysis provides evidence that individuals with relapsed or refractory NLPHL have a generally favorable prognosis. Different second-line approaches were shown to be active. The most appropriate salvage therapy for the individual patient should be chosen on the basis of factors such as the time interval between the initial NLPHL diagnosis and disease recurrence, previous treatment, and age at relapse or primary disease progression.
Presented in part orally at the 58th annual meeting of the American Society of Hematology, San Diego, CA, 3-6 December 2016.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Authorship
Contribution: D.A.E., A.P., L.S., and A.E. designed research and analyzed and interpreted data; D.A.E., A.P., L.S., M.F., B.B., B.v.T., V.D., P.B., and A.E. provided study material or patients; D.A.E., A.P., and A.E. wrote the paper; and all authors collected and assembled data and provided final approval of the manuscript
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Andreas Engert, First Department of Internal Medicine, University Hospital Cologne, Kerpener Str 62, D-50937 Cologne, Germany; e-mail: a.engert@uni-koeln.de.