Key Points
Cytoreduction with obinutuzumab and ibrutinib followed by the addition of venetoclax has acceptable safety with no tumor lysis syndrome.
This combination has preliminary activity including complete remissions with undetectable residual disease in relapsed or refractory CLL.

Abstract
Targeted therapies including the engineered afucosylated anti-CD20 monoclonal antibody obinutuzumab, Bruton’s tyrosine kinase inhibitor ibrutinib, and B-cell lymphoma protein 2 inhibitor venetoclax have demonstrated significant clinical activity in chronic lymphocytic leukemia (CLL) and, based on their complementary mechanisms, are ideal for combination. However, combining venetoclax with other active agents raises safety concerns, as it may increase the risk for tumor lysis syndrome. To minimize this risk, we designed and implemented a fixed-duration regimen using sequentially administered obinutuzumab followed by ibrutinib (cycle 2) and venetoclax (cycle 3), for a total of fourteen 28-day cycles. This phase 1b study included 12 patients with relapsed or refractory CLL. We tested 3 dose levels of venetoclax and identified the doses of all 3 agents approved by the US Food and Drug Administration for use in the combination. Adverse events were consistent with known toxicities of the individual agents, with hematologic adverse events being most frequent. No clinically significant tumor lysis syndrome occurred. The overall response rate was 92% (95% confidence interval, 62%-100%), with 42% (5/12) achieving a complete remission or complete remission with incomplete marrow recovery. There were 6 patients with no detectable CLL in both the blood and bone marrow at the end of treatment. We found this regimen to be safe and tolerable in CLL, and capable of inducing deep responses, justifying future study in our ongoing phase 2 cohorts of relapsed or refractory and treatment-naive patients, as well as larger phase 3 trials currently in planning. This trial was registered at www.clinicaltrials.gov as #NCT02427451.
Introduction
The development of targeted agents in chronic lymphocytic leukemia (CLL) has revolutionized treatment by offering high response rates regardless of cytogenetic risk category, and improved toxicity compared with standard chemoimmunotherapy.1-3 Yet, challenges remain, as these agents are not curative, patients develop resistance, and continuous treatment is required with monotherapy.4,5 To better use these novel agents, we designed a phase 1b study evaluating the combination of obinutuzumab, ibrutinib, and venetoclax. This study combines 3 highly effective agents with distinct and complementary mechanisms of action with a goal of achieving high rates of minimal residual disease (MRD) undetectable complete remission (CR) with a fixed-duration regimen, thereby allowing treatment cessation.
Ibrutinib, an inhibitor of Bruton’s tyrosine kinase in the B-cell receptor signaling cascade, and venetoclax, which specifically inhibits B-cell lymphoma protein 2, an antiapoptotic protein, both have high response rates as single agents and demonstrated complementary mechanisms in preclinical testing.2-4,6-8 Inclusion of an anti-CD20 monoclonal antibody was justified, as this class of drug improves overall survival when combined with chemotherapy.9,10 Obinutuzumab was selected, as it is superior to rituximab when used in combination with chlorambucil and has excellent single-agent activity in CLL.11,12
Dosing of the agents was as per their US label, with 3 different doses of venetoclax tested and the highest being the approved dose of venetoclax in CLL. The dosing scheme was designed to maximize benefit and safety by starting drugs sequentially during the first 3 cycles. Obinutuzumab was introduced first to avoid initial combination with ibrutinib, which has been shown to antagonize NK-cell-mediated cytotoxicity with the anti-CD20 monoclonal antibody rituximab.13-15 Initiating obinutuzumab first also allowed for maximal reduction in tumor burden, and therefore tumor lysis syndrome (TLS) risk as dosing is most dense during the first cycle. Ibrutinib was started in the second cycle and further decreased TLS risk before venetoclax dose ramp-up at the beginning of cycle 3. This phase 1b study identified the dose of venetoclax for use in this combination, with the other 2 agents fixed at the standard dose, and evaluated the feasibility, safety, and preliminary activity of this regimen in CLL.
Methods
The study was conducted at The Ohio State University and titled “Bcl-2 Inhibitor GDC-0199 in Combination with Obinutuzumab and Ibrutinib in Treating Patients With Relapsed, Refractory, or Previously Untreated Chronic Lymphocytic Leukemia” (NCT02427451). The study was approved by the Cancer Institutional Review Board, and all patients signed written informed consent.
Eligible patients were at least 18 years of age, with a diagnosis of CLL, and required treatment. All patients had received at least 1 prior treatment. Patients were required to have adequate bone marrow function, defined as a hemoglobin level of at least 8 g/dL, absolute neutrophil count of at least 1 × 109/L, and platelet count of at least 40 × 109/L, independent of growth factor support at screening unless cytopenias were clearly a result of bone marrow involvement by CLL. Patients were required to have a serum creatinine of less than 2.0 mg/dL or a creatinine clearance of at least 50 mL/min/1.73 m2, as calculated by the modified Cockcroft-Gault equation. Patients with clinical ibrutinib resistance, a Bruton’s tyrosine kinase C481S mutation, or prior toxicity other than thrombocytopenia from B-cell lymphoma protein 2 family protein inhibitors were excluded.
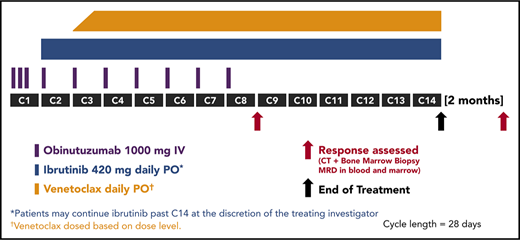
Study treatment was given for 14 cycles of 28 days, with midtherapy response assessment after cycle 8 and posttreatment response assessment 2 months after cycle 14 (supplemental Figure 1, available on the Blood Web site). Agents were started during the first 3 cycles of therapy. Obinutuzumab was given at a dose of 1000 mg intravenously on days 1 to 2 (100 mg day 1 and 900 mg day 2), 8, and 15 of cycle 1, and day 1 of cycles 2 to 8. Ibrutinib 420 mg oral daily was given days 1 to 28 of cycles 2 to 14. Venetoclax was started day 1 of cycle 3 at 20 mg oral daily with intrapatient dose ramp-up every 7 days according to US prescribing information, until the target dose was reached (supplemental Table 1). The protocol was amended to allow continuation of single-agent ibrutinib after cycle 14 at the discretion of the treating investigator. Risk for TLS was assessed at screening, according to venetoclax US prescribing information, with TLS prophylaxis and hospitalization according to individual patient risk. Patients could be admitted to the hospital for close monitoring at the treating investigator’s discretion, as this regimen had not been previously tested.
The primary objective was to determine the dose of venetoclax for use with obinutuzumab and ibrutinib at their standard doses. A 3+3 design was used for the dose levels of venetoclax, and the dose-limiting toxicity observation period was cycle 3. Adverse events were assessed and graded using the National Cancer Institute Common Terminology Criteria for Adverse Events v4.03, and were tabulated in summary form. Response at both midtherapy and end of treatment was determined according to International Workshop on Chronic Lymphocytic Leukemia 2008 criteria with MRD testing in the blood and bone marrow, using 10-color flow cytometry with a detection limit of less than 1 × 10−4.16 Responses were confirmed independently by 2 investigators (K.A.R. and J.C.B.). Response rate was provided with an exact 95% binomial confidence interval. Progression-free survival was defined as the time from start of treatment until the earlier of disease progression or death from any cause, censoring patients alive at the last known clinical assessment, and was summarized by the Kaplan-Meier method. The data were analyzed by the authors, and all authors had access to the primary data.
Results
Twelve patients were enrolled in the phase 1b feasibility study. Baseline characteristics are found in Table 1. The cohort was relatively young, with a median age of 57 years, and was not heavily pretreated, as the median number of prior treatments was 1 (range, 1-7).
There were no dose-limiting toxicities, and the highest dose level was reached, establishing venetoclax 400 mg as the dose for this combination. No patients required dose reduction or omission of obinutuzumab doses because of toxicity during any cycle. All patients completed 14 treatment cycles, with 6 continuing ibrutinib beyond cycle 14.
Treatment-related adverse events were similar to the known toxicity profiles of the individual agents (Table 2). Hematologic adverse events were most frequent, with neutropenia occurring in 10 of 12 patients and thrombocytopenia in 9 of 12. Grade 3 or 4 neutropenia occurred in 4 of 12 patients.
The most frequent nonhematologic adverse events of any grade were infusion-related reactions (10/12), bruising (9/12), diarrhea (8/12), hypertension (8/12), myalgia (7/12), and arthralgia (6/12). High-grade events were infrequent, aside from hypertension, which occurred in 3 of 12 patients. Although infusion-related reactions were frequent, only 1 was grade 3 or 4. Despite high rates of neutropenia, there were no episodes of neutropenic fever and no grade 3 or 4 infectious adverse events attributed to study treatment. One patient experienced fever and 1 had a gum infection and an upper respiratory infection, all grade 1 or 2. There were no cases of clinical or laboratory tumor lysis syndrome. All adverse events and treatment-related adverse events are found in supplemental Tables 2 and 3, respectively.
At the midtherapy response assessment after cycle 8, all 12 patients had an objective response, with 2 achieving a complete remission with incomplete marrow recovery (CRi) and 10 achieving a partial remission (PR). Four patients had no detectable MRD in both the blood and bone marrow by high-sensitivity flow cytometry at midtherapy assessment.
The overall response rate at the end of treatment assessment 2 months after cycle 14 was 92% (95% confidence interval, 62%-100%), with 11 of 12 patients responding: 4 CR, 1 CRi, 6 PR. Response deepened with continued treatment as more patients achieved CR compared with midtherapy. By the end of the treatment assessment, all 12 patients became MRD undetectable in either the blood or bone marrow, with 6 patients (3 CR and 3 PR) having no detectable MRD in both the blood and bone marrow (Figure 1; supplemental Table 4). All CRs with undetectable MRD in both compartments occurred at the highest dose level.

Treatment responses with minimal residual disease status. MRD was assessed by 10-color flow cytometry at both planned response assessments: midtherapy after cycle 8 (A) and end of treatment 2 months after completion of cycle 14 (B). The limit of detection for MRD is less than 1 × 10−4. BM, bone marrow; PB, peripheral blood.
Treatment responses with minimal residual disease status. MRD was assessed by 10-color flow cytometry at both planned response assessments: midtherapy after cycle 8 (A) and end of treatment 2 months after completion of cycle 14 (B). The limit of detection for MRD is less than 1 × 10−4. BM, bone marrow; PB, peripheral blood.
One patient treated at the lowest dose level had achieved a PR at midtherapy and then developed progressive disease at posttreatment assessment because of increased retroperitoneal lymphadenopathy. This was the most heavily pretreated patient, with 7 prior CLL therapies. Bone marrow biopsy at the end of treatment assessment 2 months after therapy discontinuation had no morphologic involvement by CLL but had detectable CLL by flow cytometry (2% of lymphocytes) and no detectable CLL in the blood. This patient was restarted on single-agent ibrutinib with continued clinical response at last follow-up more than 12 months after restarting ibrutinib.
Six patients continued on single-agent ibrutinib, including 4 with PR, 1 CR, and 1 CRi. Of those 6 patients, 3 had no detectable disease in both the blood and bone marrow. At a median duration of follow-up of 24.4 months, the estimated 24-month PFS was 92% (95% confidence interval, 54%-99%; supplemental Figure 2). All patients were alive at last follow-up.
Discussion
The advances achieved with continuous ibrutinib monotherapy or fixed-duration combination rituximab and venetoclax have transformed CLL treatment and outcomes.4,17 This progress has fostered current efforts to combine highly effective targeted agents and test the hypothesis that deep responses might facilitate therapy discontinuation. Our phase 1b study demonstrates that combination therapy with obinutuzumab, ibrutinib, and venetoclax is safe and feasible in patients with CLL, has a high overall response rate, and is capable of eliminating MRD.
There are some major advances with this regimen, including the dosing strategy. Starting obinutuzumab and ibrutinib during the first 2 cycles of treatment sufficiently reduced tumor burden so that no patients experienced TLS with venetoclax and allowed venetoclax to be started after a relatively short lead-in treatment. In addition, this regimen was overall tolerable, with all patients completing treatment without dose reduction. The most common nonhematologic toxicity was infusion-related reactions, and starting ibrutinib before obinutuzumab may also be worthy of further exploration in future trials.
There are limitations to the results of our study, such as the small sample size, and larger studies with this regimen will be needed to determine the full toxicity profile and response rates. As half the patients were continued on ibrutinib after completion of combination treatment, determination of the PFS after discontinuation of therapy will require a larger number of patients, as well as longer follow-up.
The results of this study are sufficient to justify further pursuit of this novel triplet combination. There are ongoing phase 2 cohorts at our institution to gather further data regarding efficacy and toxicity with this regimen in both treatment-naive and relapsed or refractory patients, respectively.18 Phase 3 trials with this regimen are now being initiated by the US Cooperative Groups.
Presented in abstract form at the 58th annual meeting of the American Society of Hematology, San Diego, CA, 6 December 2016.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
The authors acknowledge the members of the study team at The Ohio State University for their dedication to this study. The authors thank the clinical teams who provided care for the study patients, as well as participating patients and their supporters.
The authors acknowledge Genentech for funding this study. Work in this trial supported in part by funding from the Four Winds Foundation, Leukemia and Lymphoma Society, Vysis Inc. (part of Abbott Molecular), and the National Institutes of Health, National Cancer Institute (R01 CA177292 and R35 CA197734 to J.C.B.). Research reported in this publication was supported in part by the Ohio State University Comprehensive Cancer Center and the National Institutes of Health, National Cancer Institute under grant number P30 CA016058.
Authorship
Contribution: A.S.R., J.A.J., and J.C.B. designed the study; K.A.R., F.T.A., C.H., K.J.M., M.E.M., M.A.R., M.L., J.A.W., W.T.W., J.A.J., and J.C.B. conducted the study and treated study participants; Y.H. and A.S.R. performed the statistical analysis; N.A.H. and G.L. contributed the cytogenetic and flow cytometry minimal residual disease data; K.A.R. prepared the manuscript and figures for publication; and all authors analyzed the data, reviewed the manuscript, and agreed to its submission for publication.
Conflict-of-interest disclosure: K.A.R. receives research funding from Genentech. F.T.A. has consulted for AbbVie, Gilead Sciences, and Janssen and receives research funding from Pharmacyclics. G.L. receives research funding from Genentech. K.J.M. has received research funding from Pharmacyclics, Novartis, Merck, and BMS and has consulted for Pharmacyclics, Janssen, Genentech, BMS, and Acerta. J.A.W. received honoraria from Janssen, has consulted for Janssen, and receives research funding from MorphoSys, Karyopharm Therapeutics, and AbbVie. J.A.J. is employed by Celgene Corporation and has consulted for Genentech, Roche, AbbVie, and Pharmacyclics. J.C.B. receives research funding from Genentech, Acerta, Pharmacyclics, and Janssen. The remaining authors declare no competing financial interests.
Correspondence: Kerry A. Rogers, Division of Hematology, The Ohio State University, 458 CCC/Wiseman Hall, 410 W 12th Ave, Columbus, OH 43210; e-mail: kerry.rogers@osumc.edu.