

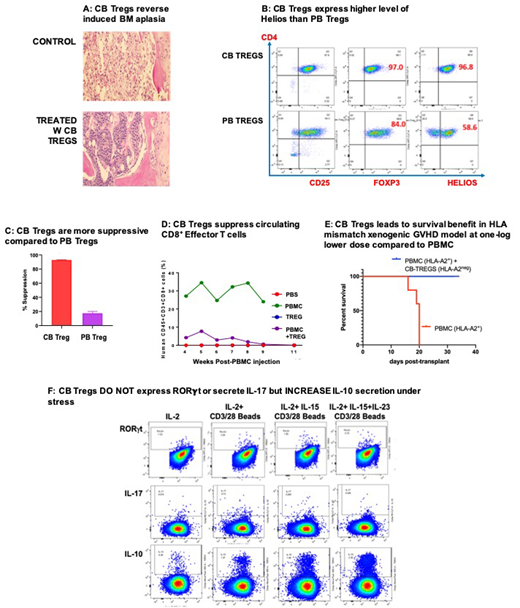
Background: Aplastic anemia is an autoimmune disease of the bone marrow (BM) characterized by defective and decreased regulatory T cells (Tregs) which results in unchecked cytotoxic T cell mediated bone marrow suppression [1]. In a xenogeneic model of induce BM aplasia, adoptive therapy with cord blood (CB) Tregs reverses such a defect (Fig 1A). Furthermore, as compared to peripheral blood (PB), CB Tregs show a higher expression of Helios, a marker of thymic derived Tregs (Fig 1B) and CB Tregs exert a superior suppression of proliferating conventional T-cells in CFSE assay (Fig 1C). In a xenogeneic mouse model of GVHD, CB Tregs can exert suppression across HLA barrier resulting in survival benefit (Fig 1D); and in another xenogenic lupus model, a single dose of CB Tregs results in significant decrease in circulating effector T cells (Fig 1E) up to 8 weeks. Furthermore, under stressful conditions of continued culture in the presence of inflammatory cytokines including IL15 and IL23, CB Tregs do not secrete IL-17 or express RORγt, a concern of plasticity that plagues PB Tregs (Fig 1F). In fact, CB Tregs increase their secretion of the suppressor cytokine, IL-10 in response to inflammatory stress, which supports our hypothesis, that CB Tregs based adoptive therapy can have wide application and can be used to treat inflammatory disorders. Therefore, we hypothesized that adoptive therapy with CB Tregs can be utilized as treatment for the inflammatory bone marrow failure (BMF) disorders including aplastic anemia, hypoplastic myelodysplasia and primary myelofibrosis.
Study Design and Methods: We have now launched a phase I clinical trial examining the role of single infusion of CK0801, an allogeneic, fresh CB Treg product, utilizing novel process development that consist of well-defined qualification criteria for the starting material (cord blood units), parameters for manufacturing and culture-expansion; and well-defined analytic testing and lot release criteria, for the treatment of BMF, where 3 doses are examined: i) dose level I: 1x106 cells/kg; ii) dose level II: 3x106 cells/kg and iii) dose level III: 10x106 cells/kg (NCT03773393). The study follows 3+3 phase I design where 3 patients will be treated at dose level I. If no DLT is observed, then the dose will be escalated to dose level II and if no DLT is observed, then the dose will be escalated to dose level III. If 1 DLT is observed at a dose level, then 3 additional patients will be treated at that level. If no additional DLTs, then that dose level will be defined as MTD. If ≥2DLTs are observed at dose level II or III, then prior dose level is defined as MTD. If ≥2DLTs at dose level I, then DSMB will review and evaluate for study continuation. MTD will be decided when 6 patients are treated at a dose level with < 2 DLTs. The eligibility criteria include: i) diagnosis of aplastic anemia, myelodysplastic syndrome or myelofibrosis, ii) Age > 18 years, iii) cord blood unit matched at HLA 3 out of 6 with the patient for generation of CK0801. The primary endpoint includes dose limiting toxicity (DLT) as defined by i) severe (grade 3 or 4) infusion toxicity within 24 hours; ii) regimen related death within 30 days or iii) severe (grade 3 or 4) cytokine release syndrome within 30 days. The secondary endpoints include i) disease-specific response including complete remission, transfusion independence and hematologic improvement and ii) duration of response. The exploratory endpoints include assessment of PB and BM immune reconstitution and inflammatory cytokines at baseline and scheduled follow ups of Days 0, +1, +3, +7, +14, +21, +30, +60, +90, +180 and +365 in the post-treatment setting. These studies will include T cell compartment analysis: Treg, Effector T cells, T-cell anti-viral activity. Serum will be analyzed for inflammatory cytokines: IL1, IL2, IL4, IL6, IL7, IL8, IL10, IL17, IFN-gamma, ST2, REG3a, OPN, Follistatin, Elafin, TGF-beta. Optional exploratory cytokines: SCF, G-CSF, GM-CSF, HGF, VEGF, SDF1a, MCP1, MCP2, TARC, MIP3a, TECK, CTACK, CCL28, FGF, PDGF, EGF, TGF-α, TLR.
The first patient is already consented with a planned total of 9 patients.
References:
1. Kordasti S, Costantini B, Seidl T, et al., Deep phenotyping of Tregs identifies an immune signature for idiopathic aplastic anemia and predicts response to treatment. 2016 Sep 1;128(9):1193-205
Kadia:AbbVie: Consultancy, Research Funding; Amgen: Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; Bioline RX: Research Funding; Celgene: Research Funding; Jazz: Membership on an entity's Board of Directors or advisory committees, Research Funding; Genentech: Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding; Pharmacyclics: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees. DiNardo:abbvie: Consultancy, Honoraria; agios: Consultancy, Honoraria; celgene: Consultancy, Honoraria; daiichi sankyo: Honoraria; jazz: Honoraria; medimmune: Honoraria; syros: Honoraria; notable labs: Membership on an entity's Board of Directors or advisory committees. Parmar:Cellenkos Inc.: Equity Ownership, Membership on an entity's Board of Directors or advisory committees, Research Funding. Iyer:Rhizen: Research Funding; Seattle Genetics: Research Funding; Trillium Therapeutics: Research Funding; Merck: Research Funding; Spectrum: Research Funding. Hari:Celgene: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Research Funding; Janssen: Consultancy, Honoraria; Kite: Consultancy, Honoraria; Amgen: Research Funding; Spectrum: Consultancy, Research Funding; Sanofi: Honoraria, Research Funding; Cell Vault: Equity Ownership; AbbVie: Consultancy, Honoraria. Jabbour:BMS: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Cyclacel LTD: Research Funding. Borthakur:Novartis: Research Funding; Xbiotech USA: Research Funding; Oncoceutics: Research Funding; Agensys: Research Funding; Janssen: Research Funding; Incyte: Research Funding; AbbVie: Research Funding; BMS: Research Funding; AstraZeneca: Research Funding; Bayer Healthcare AG: Research Funding; Eisai: Research Funding; Strategia Therapeutics: Research Funding; BioTheryX: Membership on an entity's Board of Directors or advisory committees; Argenx: Membership on an entity's Board of Directors or advisory committees; FTC Therapeutics: Membership on an entity's Board of Directors or advisory committees; Merck: Research Funding; Arvinas: Research Funding; Polaris: Research Funding; BioLine Rx: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Tetralogic Pharmaceuticals: Research Funding; PTC Therapeutics: Consultancy; Oncoceutics, Inc.: Research Funding; Eli Lilly and Co.: Research Funding; GSK: Research Funding; NKarta: Consultancy; Cantargia AB: Research Funding; Cyclacel: Research Funding. Verstovsek:Incyte: Research Funding; Roche: Research Funding; NS Pharma: Research Funding; Celgene: Consultancy, Research Funding; Gilead: Research Funding; Promedior: Research Funding; CTI BioPharma Corp: Research Funding; Genetech: Research Funding; Blueprint Medicines Corp: Research Funding; Novartis: Consultancy, Research Funding; Sierra Oncology: Research Funding; Pharma Essentia: Research Funding; Astrazeneca: Research Funding; Ital Pharma: Research Funding; Protaganist Therapeutics: Research Funding; Constellation: Consultancy; Pragmatist: Consultancy.

