

Background:
Immunomodulatory (IMiD) compounds are effective therapies for multiple myeloma (MM) acting via modulation of the CUL4 E3-ubiquitin ligase cereblon. Based on their structure individual IMiD compounds have different substrate specificities altering both their efficacy and side effect profile. These mechanistic differences impact the optimum sequencing of these agents as induction and maintenance. Within the UK NCRI Myeloma XI trial we compared triplet induction regimens containing Lenalidomide (Len) or Thalidomide (Thal) and maintenance treatment with Len or observation. With extensive long term follow up data we have explored the interaction of the induction and maintenance use of Thal and Len before and after ASCT.
Methods:
Myeloma XI is a multicenter, randomized controlled trial for newly diagnosed MM, with pathways for transplant eligible (TE) and non-eligible patients. TE patients were randomized between Len or Thal plus cyclophosphamide and dexamethasone (CRD vs CTD) continued for a minimum of 4 cycles and to max. response. For patients with a suboptimal response there was a subsequent randomization to intensification with a proteasome inhibitor containing triplet or no further therapy prior to ASCT. A maintenance randomization at 3 months post ASCT compared Len till disease progression vs observation (Obs). Analyses by molecular risk strata were pre-specified in the protocol. Adverse cytogenetic abnormalities were defined as gain(1q), t(4;14), t(14;16), t(14;20), or del(17p): standard risk (SR, no adverse cytogenetic abnormalities), high risk (HiR, one adverse cytogenetic abnormality), or ultra-high risk (UHiR, two or more adverse cytogenetic abnormalities).
Results:
2042 TE patients were randomized to CRD n=1021 and CTD n=1021. After a median follow up of 68 months (interquartile range 49-83) for the induction randomization, 1378 PFS and 728 OS primary endpoint events had occurred. Patients received a median (range) of 5 (1-18) cycles of CRD and 5 (1-13) cycles of CTD induction therapy. There were higher rates of haematological toxicity with CRD and peripheral neuropathy with CTD.
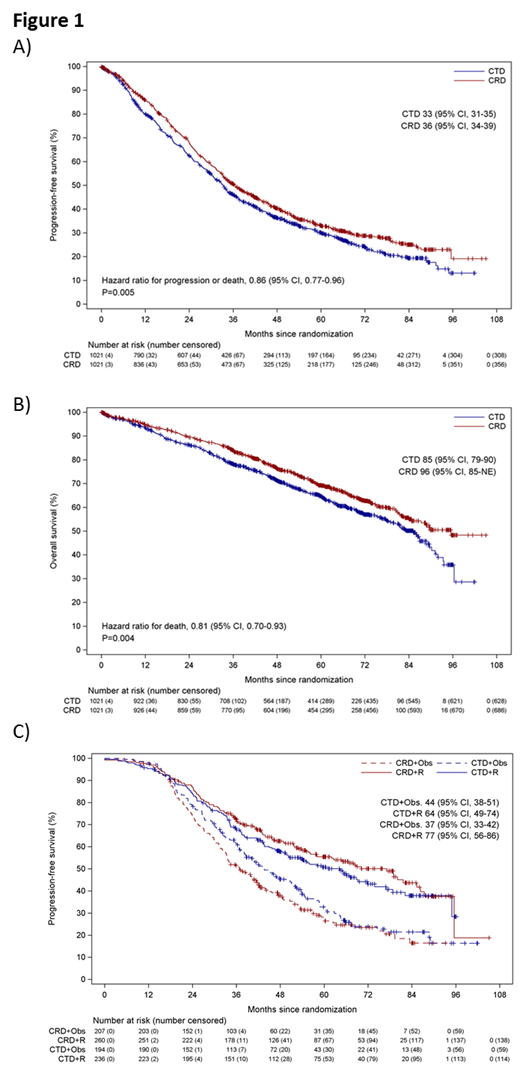
CRD induction was associated with a significantly improved median PFS (hazard ratio (HR) 0.86, 95%CI 0.77, 0.96, CRD 36 months vs CTD 33 months, P=0.005, Figure 1A) and median OS (HR 0.81, 95%CI 0.70, 0.93, CRD 96 months vs CTD 85 months, P=0.004, Figure 1B). Responses were deeper with CRD (>=VGPR 65.3%, PR 24.5%) than CTD (>=VGPR 52.8%, PR 33.2%) and depth of response was associated with outcome. Significant heterogeneity in PFS outcome was identified between molecular risk groups with HiR and UHiR benefiting most from induction with CRD rather than CTD (SR HR 0.99 [95%CI 0.79, 1.24], HiR HR 0.58 [0.44, 0.78], UHiR HR 0.60 [0.38, 0.94], P.het 0.01).
897 TE patients were randomized to Len (n=496) and Obs (n=401). After a median follow up of 68 months (interquartile range 51-84) for the maintenance randomization, 527 PFS primary endpoint events had occurred. Lenalidomide was associated with a significant improvement in PFS compared to observation (median PFS Len 64 [54,76] vs Obs 32 [28,36], HR 0.52 [0.45,0.61], P<0.001). This was consistent across all risk subgroups (SR HR 0.44 [95%CI 0.34, 0.56], HiR HR 0.50 [0.37, 0.67], UHiR HR 0.52 [0.31, 0.87], P. het 0.87).
Optimum outcomes were seen in those receiving Len as both induction and maintenance therapy (Figure 1C). Patients receiving CRD induction followed by Len maintenance (CRD-R) had a median PFS of 77 months [56, 86] compared to CTD-R 64 [49, 74], CRD-Obs 37 [33, 42] and CTD-Obs 44 [38, 51].
Conclusions:
In this study the use of Len as both induction and maintenance was associated with the best outcomes irrespective of cytogenetic risk group. With long term follow up CRD induction for newly diagnosed transplant eligible myeloma patients was associated with both a PFS and OS benefit compared to CTD and was better tolerated. The PFS impact of CRD was particularly notable in patients with high and ultra-high risk disease. Lenalidomide maintenance was associated with significantly longer PFS than observation across all risk groups.
on behalf of the NCRI Haematological Oncology Clinical Studies Group
Jackson:Celgene, Amgen, Roche, Janssen, Sanofi: Honoraria. Pawlyn:Amgen, Celgene, Janssen, Oncopeptides: Honoraria; Amgen, Celgene, Takeda: Consultancy; Amgen, Janssen, Celgene, Takeda: Other: Travel expenses. Cairns:Celgene, Amgen, Merck, Takeda: Other: Research Funding to Institution. Jones:Celgene: Honoraria, Research Funding. Kishore:Celgene, Takeda, Janssen: Honoraria, Speakers Bureau; Celgene, Jazz, Takeda: Other: Travel expenses. Garg:Janssen, Takeda, Novartis: Other: Travel expenses; Janssen: Honoraria; Novartis, Janssen: Research Funding. Lindsay:Celgene: Other: personal fees and non-financial support ; Takeda: Other: personal fees and non-financial support ; Amgen: Other: non-financial support. Russell:Jazz: Consultancy, Honoraria, Speakers Bureau; Pfizer Inc: Consultancy, Honoraria, Speakers Bureau; DSI: Consultancy, Honoraria, Speakers Bureau; Astellas: Consultancy, Honoraria, Speakers Bureau. Jenner:Abbvie, Amgen, Celgene, Novartis, Janssen, Sanofi Genzyme, Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Cook:Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Karyopharm: Consultancy, Honoraria, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Sanofi: Consultancy, Honoraria, Speakers Bureau; Takeda: Consultancy, Honoraria, Research Funding, Speakers Bureau. Drayson:Abingdon Health: Consultancy, Equity Ownership. Owen:Janssen: Other: Travel expenses; Celgene, Janssen: Honoraria; Celgene, Janssen: Consultancy; Celgene: Research Funding. Gregory:Abbvie, Janssen: Honoraria; Celgene: Consultancy, Research Funding; Amgen, Merck: Research Funding. Kaiser:Takeda, Janssen, Celgene, Amgen: Honoraria, Other: Travel Expenses; Celgene, Janssen: Research Funding; Abbvie, Celgene, Takeda, Janssen, Amgen, Abbvie, Karyopharm: Consultancy. Davies:Amgen, Celgene, Janssen, Oncopeptides, Roche, Takeda: Membership on an entity's Board of Directors or advisory committees, Other: Consultant/Advisor; Janssen, Celgene: Other: Research Grant, Research Funding. Morgan:Bristol-Myers Squibb, Celgene Corporation, Takeda: Consultancy, Honoraria; Amgen, Janssen, Takeda, Celgene Corporation: Other: Travel expenses; Celgene Corporation, Janssen: Research Funding.
CTD/CRD induction therapy and Lenalidomide maintenance 10mg 21/28 days

