

Introduction: There are multiple mechanisms of occurrence of TMA. Some of the etiologies are associated with high morbidity and mortality, but there are very subtle differences in presentation. A high index of suspicion is recommended for thrombotic thrombocytopenic purpura (TTP) due to the time sensitive nature of treatment initiation and poor outcomes associated with delay in treatment. Due to this, treatment with PLEX is often initiated empirically before diagnostic test results are available. We aim to report the management and outcomes of TMA along with the predictive value of the PLASMIC score in our patient population, over a 10-year period in an inner-city safety net hospital.
Methods: This is a single center observational study including patients who underwent PLEX for a diagnosis of TMA, due to concern for TTP between January 2009 and May 2019 at an inner-city safety net hospital. Patients were identified from blood bank records and data was collected by review of electronic medical record. We excluded patients <18 years old and who received PLEX for indications other than that described previously. Data was collected until death or last follow-up. Statistical analysis was done using STATA.
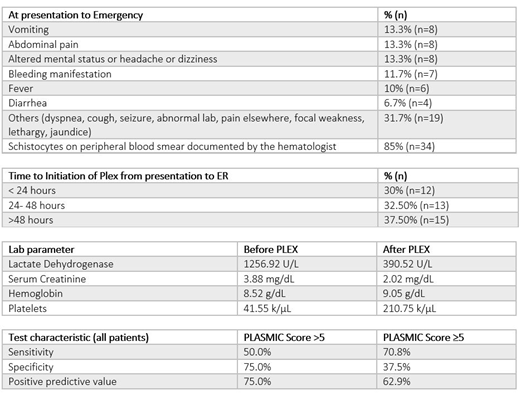
Results: A total of 40 patients met the inclusion criteria. Of these, 57.5% (n=23) were male, 17.5% (n=7) had a known malignancy and 15% (n=6) had human immunodeficiency virus infection. Study population was predominantly African American and Hispanic- comprising 75% (n=30) and 17.5% respectively- which differentiates our study from other validation studies for the PLASMIC score. Symptoms at presentation to emergency department, time to initiation of PLEX from presentation, and lab parameters before and after PLEX are shown in the attached table. ADAMTS13 activity level is available in 65% (n=26) patients, 57.7% of which were sent before initiation of PLEX. Average number of PLEX sessions during the admission was 9.4 (range: 2-30). As part of treatment, 85% (n=34) received steroids and 17.5% (n=7) received hemodialysis. 5 patients received rituximab and 2 received eculizumab. Final diagnoses included TTP in 62.5% (n=25), complement mediated TMA in 5% (n=2), drug induced TMA in 10% (n=4), TMA from sepsis or rheumatological condition in 15% (n=6), bone marrow suppression due to chemotherapy in 5% (n=2) and unsure in 2.5% (n=1). Average length of stay was 22.2 days (range: 6-85 days). Of the total 40 patients, 7.5% (n=3) died on the same admission, 10% (n=4) died after discharge and 3 were readmitted for repeat PLEX. Duration of follow-up after discharge ranged from 9 to 3319 days (mean 1102.6 days). We retrospectively estimated the PLASMIC score at the time of presentation for all the patients. Amongst the patients eventually diagnosed with TTP, 50% had a PLASMIC score of >5 and 70.83% had a score ≥5 at the time of presentation. Among non-TTP TMA, 25% had a score of >5 and 62.5% had a score ≥5. The sensitivity, specificity and positive predictive value of PLASMIC score for prediction of final diagnosis of TTP was calculated for all patients who met inclusion criteria and is shown in the attached table. Of those who underwent PLEX in the setting of TMA for the concern of TTP, only about a third were started on PLEX within 24 hours.
Conclusion:Among our study population, only about a third were started on PLEX within 24 hours which is concerning and highlights the need for quality improvement initiatives to increase provider awareness and decrease time to PLEX. Final diagnosis of TTP was made in 62.5% of the patients but notably, the performance of PLASMIC score in our patient population was inferior compared to prior validation studies. One possible explanation for this could be the difference in baseline patient demographics, with our patients belonging mostly to minority groups. There is a need for further studies with derivation and validation cohorts in this patient population to derive a scoring system that is more predictive.
No relevant conflicts of interest to declare.

