

Introduction: Allogeneic hematopoietic stem-cell transplantation (HSCT) is curative for many patients with advanced hematologic cancers, including adverse-risk acute myeloid leukemia (AML). This is principally through the induction of a graft-versus-leukemia (GVL) immune effect, mediated by donor T-cells. The incredible diversity and specificity of T-cells is due to rearrangement between V, D, and J regions and the random insertion/deletion of nucleotides, taking place in the hypervariable complementarity determining region 3 (CD3) of the T-cell receptor (TCR). Massively parallel sequencing of CDR3 allows for a detailed understanding of the T-cell repertoire, an area relatively unexplored in AML. Therefore, we sought out to characterize the T-cell repertoire in AML before and after HSCT, specifically for those with a durable remission.
Methods: We identified 45 bone marrow biopsy samples, paired pre- and post-HSCT, from 14 patients with AML in remission for > 2 years as of last follow-up. We next performed immunosequencing of the TCRβ repertoire (Adaptive Biotechnologies). DNA was amplified in a bias-controlled multiplex PCR, resulting in amplification of rearranged VDJ segments, followed by high-throughput sequencing. Resultant sequences were collapsed and filtered in order to identify and quantitate the absolute abundance of each unique TCRβ CDR3 region. We next employed various metrics to characterize changes in the TCR repertoire: (1) clonality (range: 0-1; values closer to 1 indicate a more oligoclonal repertoire), it accounts for both the number of unique clonotypes and the extent to which a few clonotypes dominate the repertoire; (2) richness with a higher number indicating a more diverse repertoire with more unique rearrangements); (3) overlap (range: 0-1; with 1 being an identical T-cell repertoire). All calculations were done using the ImmunoSeq Analyzer software.
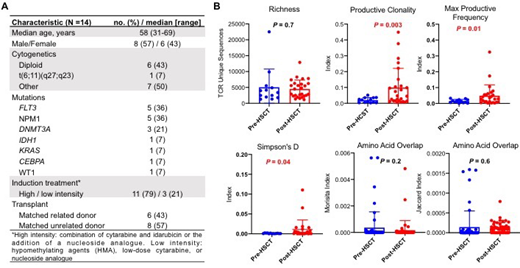
Results: The median age of patients included in this cohort was 58 years (range: 31-69). Six patient (43%) had a matched related donor, and 8 (57%) had a matched unrelated donor. Baseline characteristics are summarized in Figure 1A. Six samples were excluded from further analysis due to quality. TCR richness did not differ comparing pre- and post-HSCT, with a median number pre-HSCT of 3566 unique sequences (range: 1282-22509) vs 3720 (range: 1540-12879) post-HSCT (P = 0.7). In order to assess whether there was expansion of certain T-cell clones following HSCT, we employed several metrics and all were indicative of an increase in clonality (Figure 2B). Productive clonality, a measure of reactivity, was significantly higher in post-transplant samples (0.09 vs 0.02, P = 0.003). This is a measure that would predict expansion of sequences likely to produce functional TCRs. The Maximum Productive Frequency Index was higher post-HSCT indicating that the increase in clonality was driven by the top clone (most prevalent per sample). Similarly for the Simpson's Dominance index, another marker of clonality which was higher post-HSCT (0.01 vs 0.0009, P = 0.04). In order to determine whether this clonal expansion was driven by TCR clones shared among patients, we compared the degree of overlap in unique sequences among pre and post-HSCT samples. We found there was very little overlap between samples in the pre and the post-transplant setting and no change in the Morisita and Jaccard Overlap Indices.
Conclusions: In conclusion, we show in this analysis an increase in clonality of T-cells following HSCT in patients with AML. This is likely related to the GVL effect after recognition of leukemia antigens by donor T cells and subsequent expansion of these T-cells. These expanded T-cell clonotypes were unlikely to be shared by patients in this cohort, likely reflecting the variety of antigens leading to the GVL effect. This could have direct implications on TCR-mediated immune-therapies given the likely need for a personalized, patient-specific design for these therapies.
Kantarjian:BMS: Research Funding; Novartis: Research Funding; AbbVie: Honoraria, Research Funding; Jazz Pharma: Research Funding; Astex: Research Funding; Immunogen: Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Agios: Honoraria, Research Funding; Daiichi-Sankyo: Research Funding; Takeda: Honoraria; Amgen: Honoraria, Research Funding; Cyclacel: Research Funding; Ariad: Research Funding; Pfizer: Honoraria, Research Funding. Short:Takeda Oncology: Consultancy, Research Funding; AstraZeneca: Consultancy; Amgen: Honoraria. Cortes:Takeda: Consultancy, Research Funding; Bristol-Myers Squibb: Consultancy, Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Sun Pharma: Research Funding; BiolineRx: Consultancy; Novartis: Consultancy, Honoraria, Research Funding; Astellas Pharma: Consultancy, Honoraria, Research Funding; Merus: Consultancy, Honoraria, Research Funding; Immunogen: Consultancy, Honoraria, Research Funding; Biopath Holdings: Consultancy, Honoraria; Daiichi Sankyo: Consultancy, Honoraria, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; Forma Therapeutics: Consultancy, Honoraria, Research Funding. Jabbour:Cyclacel LTD: Research Funding; Pfizer: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; BMS: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding. Molldrem:M. D. Anderson & Astellas Pharma: Other: Royalties.

