

Introduction:
The autologous anti-CD19 chimeric antigen receptor (CAR) T-cell therapy, axicabtagene ciloleucel (Axi-cel) improved long-term survival of patients with relapsed/refractory diffuse large B-cell lymphoma (r/r DLBCL). Long-term analysis of the pivotal ZUMA-1 trial indicates a 2-year PFS of ~40% (Locke, Lancet Oncology 2018). Early identification of patients with increased relapse risk may allow for early intervention and improved outcomes. In a pilot study of 6 ZUMA-1 patients, minimal residual disease (MRD) evaluation via a next-generation sequencing MRD assay (Adaptive Biotechnologies, Seattle, WA) to assess for circulating tumor (ct)DNA, mirrored clinical outcome as assessed by PET-CT (Hossain et. al. Leukemia & Lymphoma 2019). Based on these promising results, a multi-institutional prospective study utilizing cell-free MRD assessments to predict outcomes in r/r DLBCL patients after Axi-cel therapy was initiated.
Methods:
To identify tumor clonotype(s), tumor DNA extracted from archival paraffin-embedded tissue underwent PCR amplification of IgH-VDJ, IgH-DJ and IgKappa/Lambda regions using universal consensus primers. CtDNA levels were measured pre-LD, 0, 7, 14, 21, 28, 56, 90, 180, 270, and 365 days following Axi-cel infusion. PET-CT scans were obtained at baseline, Day 28, Month 3, 6, and 12 with response assessed per Lugano criteria. Deauville 1-3 was considered PET-negative. The protocol prespecified that patients with less than Day 28 follow-up be excluded from analysis. Any detectable ctDNA was considered MRD positive.
Results:
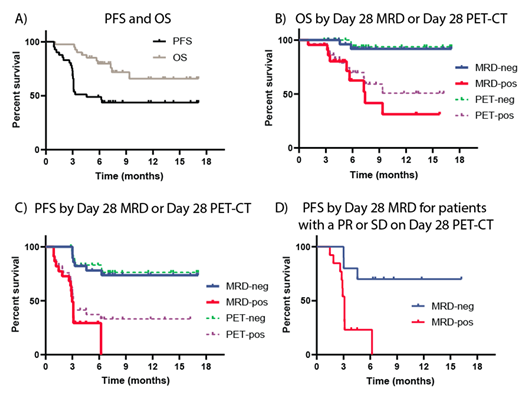
Here we report on the pre-planned analysis of the first 50 study patients with at least a Day 28 MRD assessment and 3 months of follow up. An additional 4 patients with at least 3 months of follow-up but who did not have a Day 28 MRD assessment were also included. Baseline characteristics and clinical outcomes of patients were similar to ZUMA-1 and a real-world analysis of 295 patient who received Axi-cel (Nastoupil et al ASH 2018). The median age was 61 years old (range 19-76) (53.7% male, 46.3% female) and 59% of patients received 3 or more prior lines of therapy (range 1-6). After a median follow-up of 7.5 months, the best overall response rate was 87% (47 of 54) and complete response rate was 57% (31 of 54). The median OS was not reached and median PFS was 4.6 months (panel A). At Day 28, 56% (28 of 50) of patients were MRD negative (MRD-neg) and 44% (22 of 50) were MRD positive (MRD-pos). As compared to MRD-pos, MRD-neg correlated with improved median PFS (not reached vs. 2.96 months, p<0.0001) and median OS (not reached vs.7.4 months, p=0.0005) (panels B and C). By PET assessment on Day 28, 46% (25 of 54) of patients were PET-negative (PET-neg) and 54% (28 of 54) were PET-positive (PET-pos). When compared to PET-pos patients, PET-neg patients demonstrated an improved median PFS (not reached vs. 3.1 months, p=0.0007) and median OS (both not reached, p=0.0096). MRD and PET-CT on Day 28 were able to identify patients relapsed by 6 months with similar sensitivity, 71% (95% CI: 48-89%) and 77% (95% CI: 55% to 92%), respectively. However, Day 28 MRD status had improved specificity as compared to Day 28 PET status, 94% (95% CI: 71% to 99%) versus 63% (95% CI: 38% to 83%). Day 28 MRD assessment was particularly helpful in identifying high-risk patients in the Day 28 PET-pos subgroups of patients with a PR (n=20) or SD (n=3) (panel D). This subgroup of patients with MRD-pos (n=13) had an inferior median PFS compared to those who were MRD-neg (n=10) (3.1 months vs. not reached, p=0.0033). Of note, one MRD-neg patient died without disease at 4.5 months. After excluding those (n=4) with progressive disease on Day 28 (all MRD-pos), 72% (16 of 22) of patients were MRD-pos at least 2 months prior to radiographic progression and 86% (19 of 22) were MRD-pos at least 1 month prior to radiographic progression.
Conclusion:
MRD monitoring using high-throughput sequencing of ctDNA has the potentially to make an impact on the clinical management of patients undergoing Axi-cel therapy. Furthermore, ctDNA is an informative tool to compare CAR19 therapies that vary by costimulatory domains or production methods. This technology potentially overcomes fundamental limitations of DLBCL imaging (cost, radiation exposure & limited repetition) and may minimize the need for surveillance PET-CT scans. These results provide a rationale for designing MRD-based risk-adaptive CAR T cell clinical trials.
Kirsch:Adaptive Biotechnologies: Employment. Jacob:Adaptive Biotechnologies: Employment, Other: shareholder. Mullins:Adaptive Biotechnologies: Employment. Lee:Adaptive Biotechnologies: Employment, Equity Ownership. Mackall:Obsidian: Research Funding; Lyell: Consultancy, Equity Ownership, Other: Founder, Research Funding; Nektar: Other: Scientific Advisory Board; PACT: Other: Scientific Advisory Board; Bryologyx: Other: Scientific Advisory Board; Vor: Other: Scientific Advisory Board; Roche: Other: Scientific Advisory Board; Adaptimmune LLC: Other: Scientific Advisory Board; Glaxo-Smith-Kline: Other: Scientific Advisory Board; Allogene: Equity Ownership, Membership on an entity's Board of Directors or advisory committees; Apricity Health: Equity Ownership, Membership on an entity's Board of Directors or advisory committees; Unum Therapeutics: Equity Ownership, Membership on an entity's Board of Directors or advisory committees. Locke:Cellular BioMedicine Group Inc.: Consultancy; Kite: Other: Scientific Advisor; Novartis: Other: Scientific Advisor. Miklos:Adaptive Biotechnologies: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding; Juno: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees; BMS: Membership on an entity's Board of Directors or advisory committees; Kite-Gilead: Membership on an entity's Board of Directors or advisory committees, Research Funding; AlloGene: Membership on an entity's Board of Directors or advisory committees; Precision Bioscience: Membership on an entity's Board of Directors or advisory committees; Miltenyi Biotech: Membership on an entity's Board of Directors or advisory committees; Becton Dickinson: Research Funding.

