

Despite recent developments in the therapy of chronic lymphocytic leukemia (CLL), Richter's transformation (RT), an aggressive lymphoma, remains a clinical challenge. Immune checkpoint inhibitor (ICI) therapy has shown promise in selective lymphoma types, however, only 30-40% RT patients respond to anti-PD1 pembrolizumab; while the underlying CLL failed to respond and 10% CLL patients progress rapidly within 2 months of treatment. Studies indicate pre-existing T cells in tumor biopsies are associated with a greater anti-PD1 response, hence we hypothesized that pre-existing T cell subset characteristics and regulation in anti-PD1 responders differed from those who progressed in CLL.
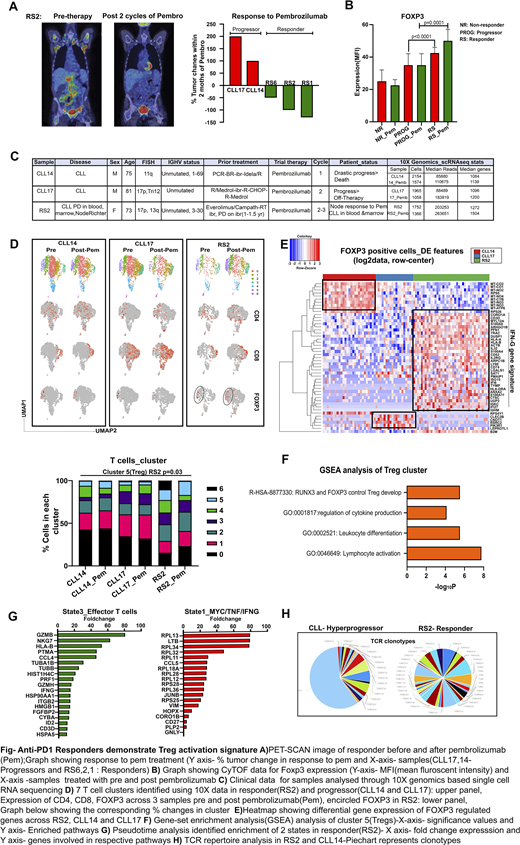
We used mass cytometry (CyTOF) to analyze T cell subsets isolated from peripheral blood mononuclear cells (PBMCs) from 19 patients with who received pembrolizumab as a single agent. PBMCs were obtained baseline(pre-therapy) and within 3 months of therapy initiation. Among this cohort, 3 patients had complete or partial response (responders), 2 patients had rapid disease progression (progressors) (Fig. A), and 14 had stable disease (non-responders) within the first 3 months of therapy. CyTOF analysis revealed that Treg subsets in responders as compared with progressors or non-responders (MFI -55 vs.30, p=0.001) at both baseline and post-therapy were increased (Fig. B). This quantitative analysis indicated an existing difference in Tregs and distinct molecular dynamic changes in response to pembrolizumab between responders and progressors.
To delineate the T cell characteristics in progressors and responders, we performed single-cell RNA-seq (SC-RNA-seq; 10X Genomics platform) using T (CD3+) cells enriched from PBMCs derived from three patients (1 responder: RS2; 2 progressors: CLL14, CLL17) before and after treatment. A total of ~10000 cells were captured and an average of 1215 genes was detected per cell. Using a clustering approach (Seurat V3.1.5), we identified 7 T cell clusters based on transcriptional signature (Fig.C). Responders had a larger fraction of Tregs (Cluster 5) as compared with progressors (p=0.03, Fig. D), and these Tregs showed an IFN-related gene signature (Fig. E).
To determine any changes in the cellular circuitry in Tregs between responders and progressors, we used FOXP3, CD25, and CD127 as markers for Tregs in our SC-RNA-seq data. We saw a greater expression of FOXP3, CD25, CD127, in RS2 in comparison to CLL17 and CLL14. Gene set enrichment analysis (GSEA) revealed the upregulation of genes involved in lymphocyte activation and FOXP3-regulated Treg development-related pathways in the responder's Tregs (Fig.F). Together, the greater expression of genes involved in Treg activation may reduce the suppressive functions of Tregs, which led to the response to anti-PD1 treatment seen in RS2 consistent with Tregs in melanoma.
To delineate any state changes in T cells between progressors and responder, we performed trajectory analysis using Monocle (R package tool) and identified enrichment of MYC/TNF/IFNG gene signature in state 1 and an effector T signature in state 3 For RS2 after treatment (p=0.003), indicating pembrolizumab induced proliferative and functional T cell signatures in the responder only. Further, our single-cell results were supported by the T cell receptor (TCR beta) repertoire analysis (Adaptive Biotechnology). As an inverse measure of TCR diversity, productive TCR clonality in CLL14 and CLL17 samples was 0.638 and 0.408 at baseline, respectively. Fifty percent of all peripheral blood T cells were represented by one large TCR clone in CLL14(progressor) suggesting tumor related T-cell clone expansion. In contrast, RS2(responder) contained a profile of diverse T cell clones with a clonality of 0.027 (Fig. H). Pembrolizumab therapy did not change the clonality of the three patients during the treatment course (data not shown).
In summary, we identified enriched Treg signatures delineating responders from progressors on pembrolizumab treatment, paradoxical to the current understanding of T cell subsets in solid tumors. However, these data are consistent with the recent observation that the presence of Tregs suggests a better prognosis in Hodgkin lymphoma, Follicular lymphoma, and other hematological malignancies.
Kay:Pharmacyclics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Oncotracker: Membership on an entity's Board of Directors or advisory committees; Rigel: Membership on an entity's Board of Directors or advisory committees; Juno Theraputics: Membership on an entity's Board of Directors or advisory committees; Agios Pharma: Membership on an entity's Board of Directors or advisory committees; Cytomx: Membership on an entity's Board of Directors or advisory committees; Astra Zeneca: Membership on an entity's Board of Directors or advisory committees; Morpho-sys: Membership on an entity's Board of Directors or advisory committees; Tolero Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees, Research Funding; Bristol Meyer Squib: Membership on an entity's Board of Directors or advisory committees, Research Funding; Acerta Pharma: Research Funding; Sunesis: Research Funding; Dava Oncology: Membership on an entity's Board of Directors or advisory committees; Abbvie: Research Funding; MEI Pharma: Research Funding. Ansell:AI Therapeutics: Research Funding; Takeda: Research Funding; Trillium: Research Funding; Affimed: Research Funding; Bristol Myers Squibb: Research Funding; Regeneron: Research Funding; Seattle Genetics: Research Funding; ADC Therapeutics: Research Funding. Ding:Astra Zeneca: Research Funding; Abbvie: Research Funding; Octapharma: Membership on an entity's Board of Directors or advisory committees; MEI Pharma: Membership on an entity's Board of Directors or advisory committees; alexion: Membership on an entity's Board of Directors or advisory committees; Beigene: Membership on an entity's Board of Directors or advisory committees; DTRM: Research Funding; Merck: Membership on an entity's Board of Directors or advisory committees, Research Funding.
pembrolizumab

