

Introduction
Although autologous CAR-T therapy targeting CD19+ B-cell has proven efficacy in hematological malignancies. The challenges such as undesirable waiting time, possible manufacturing failures and high cost, remain to be solved. In addition, antigen-loss/downregulation leads to treatment failure after single-target CAR-T therapy. To tackle these issues, we developed a universal CD19/CD22-targeting CAR-T cell with the TRAC region and CD52 gene disrupted using CRISPR/Cas9 technology. Pre-clinical data demonstrated the safety of CRISPR gene editing and the anti-leukemia ability of CTA101.
Method
Pts with CD19+ or CD22+ r/r B-ALL received a single dose of CTA101 with traditional 3+3 dose escalation (dose level: 1, 3 and 6×106 CAR+ T cells/kg). Prior to CTA101 infusion, pts received pre-conditioning chemotherapy regimen consisting of cyclophosphamide, fludarabine and alemtuzumab. The primary endpoint is the frequency of DLTs and AEs and secondary endpoints including ORR, OS, cellular PK, etc. (NCT04227015)
Results
Characteristics of CTA101
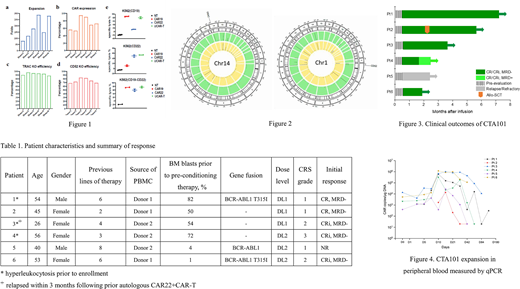
CTA101 was manufactured by electroporation of ribonucleoprotein complexes (RNP) comprising Cas9 loaded with sgRNA targeting TRAC and CD52 followed by lentiviral transduction of the CAR transgene. All products were expanded above 100-folds after 10-12 days manufacturing (Fig.1a). CAR expression was detected by FCM staining, ranging from 40~80% (Fig.1b). The frequency of editing as determined by flow cytometry was consistently above 85% (88%-97%) for TRAC and above 65% (68%-83%) for CD52 (Fig.1c, 1d).
The CD19/CD22 dual targeting universal CAR-T cells showed potent antigen specific cytotoxicity, and mitigated tumor antigen escape (Fig.1e).
Whole genome sequencing was carried out to assess the on-target and off-target editing events. While most mutations were on target, a few off-target mutations were identified, which needed further investigation (Fig.2).
QPCR assays identified no detectable rearrangements occurred with the simultaneous editing of four loci: TRAC and CD52 (TRAC-CD52) during the manufacture process. Residual Cas9 protein was quantified during the manufacturing process, showing declining levels that were 0.195 fg/cell (detection limit of sensitive ELISA) in the final product.
Clinical result
As of August 5th 2020, 8 adult pts were screened, and 6 adult pts were enrolled. All of 6 patients received one infusion of CTA101 (DL1: 3 pts; DL2: 3 pts), with no more than 8 days between enrollment and infusion. The median age of 6 pts was 49 years (range, 26 to 56), the median prior lines of therapies were 5 (range, 2 to 8), and the median marrow blast percentage was 52% (range, 1 to 82). 3 pts had hyperleukocytosis prior to enrollment with difficulties in apheresis for autologous CAR-T, 1 relapsed after autologous CD22 CAR-T, and 3 had high-risk genomic lesions (Table 1).
All 6 pts were available for evaluation of safety and efficacy. No DLTs, GvHD, ICANS and death occurred to date. All pts experienced CRS (3 G1, 2 G2, 1 G3), and the G3 CRS recovered within 7 days with one dose of tocilizumab and glucocorticoids. Other common AEs were prolonged cytopenia (3 G3), virus reactivation/infections (CMV 1 G2, 2 G3; ADV 1 G1), bacterial pneumonia (1 G3), and fungal sepsis (1 G3). The majority of events recovered to date. No replication competent lentivirus (RCL) has been detected.
On D28 after CTA101 infusion, 5/6 (83.3%) pts achieved CR/CRi, and 5/5 (100%) pts achieved MRD-. With a median follow-up of 85 days (range, 53 to 202), 4/5 pts remained MRD-, 1/5 had MRD+ CR (Fig. 3). Only 1 pt received HSCT in remission on D60.
Expansion had been observed in all pts and peaked from D10 to D14 (Fig.4). The correlation among dose level, donor difference, tumor burden and degree of expansion could not be identified. The median duration of persistence was 42 days. The lowest peak expansion was detected by qPCR in the pt without response and whose T lymphocyte recovered within D7, while FCM did not detect CTA101 expansion in the pt.
Conclusions
CTA101 demonstrates manageable safety profile and deep response of high MRD- CR/CRi rate. No GvHD and CRISPR/Cas9 genome editing associated AEs occurred. Early data of cellular PK and efficacy illustrate that CRISPR gene editing does not curtail the expansion and anti-leukemia capacity of CAR-T. Updated data, including long term gene editing-related AEs, will be presented after further follow-up.
Zhou:Nanjing Bioheng Biotech Co., Ltd: Current Employment. Ge:Nanjing Bioheng Biotech Co., Ltd: Current Employment. Han:Nanjing Bioheng Biotech Co., Ltd: Current equity holder in private company. Wang:Nanjing Bioheng Biotech Co., Ltd: Current Employment. Zhang:Nanjing Bioheng Biotech Co., Ltd: Current Employment. Ren:Nanjing Bioheng Biotech Co., Ltd: Current equity holder in private company.

