

Abstract
CD33/34 lineage specific chimerism analysis (CD33/34 LCA) can improve the predictive value of chimerism monitoring after allo-SCT in AML. Recently, real time PCR (qPCR) has been proposed for highly sensitive and accurate quantitation of chimerism. However, data to compare clinical impact of qPCR versus gold standard conventional STR-PCR was not available. In 2011, we reported on the impact of STR chimerism monitoring in a pediatric AML multicenter study (Rettinger, Willasch et al., Blood 2011;118(20):5681-88).
Hereby, we present a prospective analysis on CD33/34 LCA in bone marrow (BM) and mononuclear cell (MNC) chimerism in peripheral blood (PB) by qPCR in the pediatric AML cohort mentioned above. Pre-existing STR-PCR data were used for comparison. This analysis for the first time refers to the clinical impact of a combination of CD33/34 LCA and qPCR technology.
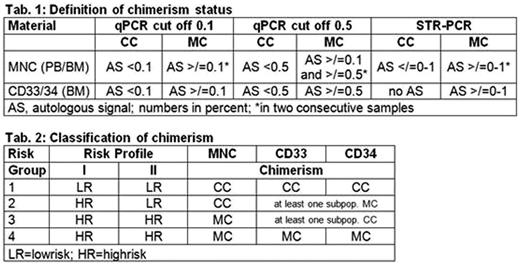
Monitoring of 75 transplantations, performed in 72 patients at 11 German pediatric transplant centers between 05/2005 and 04/2009, included 26 (0-84) PB and 5 (0-21) BM samples per patient and covered 1.5 (0.1-4.3) years (median). PB was analyzed weekly and BM at days 30, 60, 100 and 6, 9, 12, 15 and 18 months post-transplant. Lowering the quantifiable limit by qPCR (here </=10E-3 (0.1%)) can result in detection of recipient derived (autologous) signals (AS) in virtually every sample. The challenge was to define a clinically relevant cut off level for diagnosis of complete (CC) or mixed chimera (MC). For qPCR, cut off levels of 0.1 and 0.5% for AS were evaluated and chimerism was defined according to tab. 1. Based on this definition, risk groups and profiles were specified (tab. 2). Allocation into risk groups 2 to 4 was done at day of first MC in either compartment. Risk profile I (RP I) defined each sample with MC in either compartment as HR, whereas risk profile II (RP II) defined each sample with MC in MNC as HR.
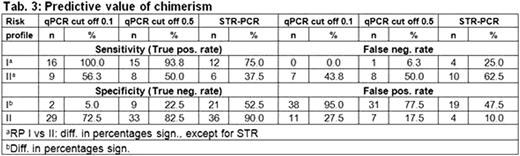
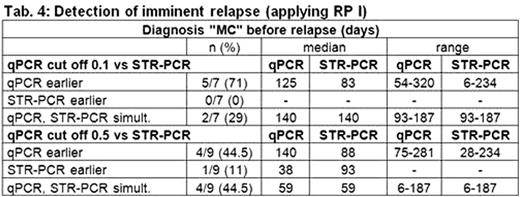
56/75 transplant follow-ups allowed for analysis of predictive value of chimerism (tab. 3). Sensitivity of RP I ranged from 100% (qPCR cut off 0.1) to 75% (STR-PCR); notably specificity was low and false pos. rate high, if this highly sensitive approach was applied. In RP II sensitivity was significantly lower compared to RP I, but specificity was considerably higher and false pos. rate lower. Relapse was predicted earlier by qPCR with a median of 42 days compared to STR-PCR in 71% if 0.1% cut off for definition of MC was applied (tab. 4). If 0.5% cut off was used, this rate dropped to 44.5%.
Taken together, qPCR as well as STR-PCR allowed for monitoring of chimerism. Each method revealed its specific pros and cons according to its high (qPCR, </=10E-3) or moderate (STR-PCR, 10E-2) quantifiable limit. For the first time we describe clinically applicable cut off levels for qPCR to define complete and mixed chimeras. LCA in CD33/34 subpopulations increased the sensitivity of chimerism monitoring. Early and sensitive detection of impending relapse was possible by qPCR. However, the substantial proportion of false positives had to be kept in mind.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal