

Abstract
Introduction:
Although allogeneic hematopoietic cell transplantation (HCT) is a potentially curative therapy for hematologic neoplasms, one of its limiting toxicities continues to be graft versus host disease, both acute and chronic (aGVHD, cGVHD). Sirolimus is a mammalian target of rapamycin (mTOR) inhibitor which has been found to be effective in GVHD prophylaxis, in combination with calcineurin inhibitors like tacrolimus. The impact of sirolimus on immune reconstitution has not been comprehensively investigated in-vivo thus far. We now present a post-hoc analysis of the randomized study BMT-CTN 0402, examining the effect of sirolimus on immune subsets post-transplant. We further examine the association between different lymphocyte subsets and outcomes post-transplant in each arm.
Methods:
BMT-CTN 0402 was a randomized trial (n=304) which compared two GVHD prophylaxis regimens, sirolimus/tacrolimus (Sir/Tac) versus tacrolimus/methotrexate (Tac/MTX), in AML/ALL/MDS patients, undergoing myeloablative HLA-matched transplantation. There was no difference in 114-day GVHD free survival (primary end-point) as well as acute or chronic GVHD, relapse or overall survival between arms. 264/304 patients had available samples for the current post-hoc analysis. Blood samples were collected at 1,3, 6, 12 and 24 months post-HCT. Multi-parameter flow cytometry was performed at the project lab (Esoterix Clinical Trials Services) in a blinded fashion, and results were compared between arms. Multivariable Cox regression models, treating each phenotypic parameter as a time dependent variable, were constructed to study impact of reconstitution on clinical outcomes.
Results:
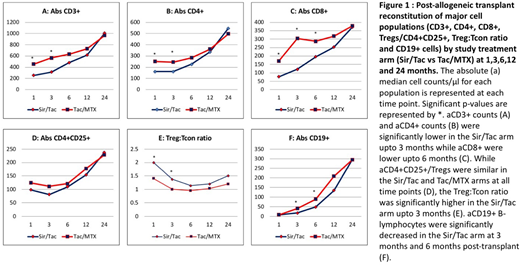
There were no significant differences in patient and transplant characteristics between the Sir/Tac and Tac/MTX arms in this analysis. Absolute lymphocyte count (ALC), CD3+ and CD4+ counts were significantly decreased in the Sir/Tac arm upto 3 months post-HCT while CD8+ cells recovered even slower (upto 6 months) in this arm (Figure 1, Panels A,B and C). Interestingly there was no difference in the absolute number of regulatory T-cells (Tregs/CD4+ CD25+) between arms at any point post-HCT (Figure 1, Panel D). However the Treg:Tcon ratio was significantly greater in the Sir/Tac arm in the first 3 months post-HCT (Figure 1, Panel E). B-lymphocyte recovery was significantly compromised in the Sir/Tac arm from 1 to 6 months post-HCT (Figure 1, Panel F) while NK cells reconstitution was not affected in the sirolimus arm. In the outcomes analysis, higher numbers of CD3+, CD4+. CD8+ and Tregs were associated with better overall survival. Neither Treg numbers nor Treg:Tcon ratio correlated with GVHD.
Conclusion:
Sir/Tac has a more profound T-cell suppressive effect than the standard of care combination of Tac/MTX in the early post-transplant period, and particularly compromises recovery of CD8+ T-cells with potential implications in the prevention of aGVHD. Sirolimus when used in-vivo with tacrolimus does not result in increased absolute numbers of Tregs, however it does have a beneficial effect on the Treg:Tcon balance in the first 3 months after transplantation, which may be important in the context of cGVHD prevention. Calcineurin-inhibitor free, sirolimus containing GVHD prophylaxis strategies, incorporating other novel agents, should be investigated further to maximize the favorable effect of sirolimus on Treg:Tcon balance in the post-transplant immune repertoire. Sirolimus significantly compromises B-cell recovery in the first 6 months post-HCT with potential complex effects on cGVHD which merit further study.
Acknowledgments:
Support for this study was provided by grant #U10HL069294 to the Blood and Marrow Transplant Clinical Trials Network from the National Heart, Lung, and Blood Institute and the National Cancer Institute, along with contributions by Wyeth Pharmaceuticals Inc. BMT CTN 0402 biospecimens were obtained from the NHLBI Biologic Specimen and Data Repository Information Coordinating Center (BioLINCC). The content is solely the responsibility of the authors and does not necessarily represent the official views of the above mentioned parties
Additional support was provided by the Division of Allergy, Immunology, and Transplantation, National Institute of Allergy and Infectious Diseases for the ancillary study, 'GVHD Prophylaxis - Immune Reconstitution.'
Soiffer:Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees. Antin:Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal