

Abstract
Introduction: Adoptive transfer of thymic derived regulatory T-cells (tTregs) or Treg type I cells that arise in the periphery can ameliorate GVHD and autoimmunity in mice. However, high Treg doses (~1:1 with donor T-cells) are required to reproducibly suppress disease. In the periphery, a population of non-Treg CD4+ T-cells can be induced to acquire a Treg phenotype and function. We defined a GMP-compliant method for selecting, inducing and expanding Tregs from peripheral blood CD4+25- T cells with IL-2, sirolimus and TGFß. Sirolimus/TGFß iTregs are as suppressive as cord blood derived tTregs and the potential yield is 50-fold higher in a 2 week culture period. We hypothesized that inducible regulatory T cells (iTregs) will be effective for acute GVHD (aGVHD) prevention without concomitantly increasing the risk of opportunistic infection and relapse.
Methods: We performed a phase I single center dose escalation study with an extension at the best available dose to determine the tolerability of inducible regulatory T cells (iTregs) given to adult patients undergoing reduced intensity HLA-identical sibling donor peripheral blood stem cell (PBSC) transplantation for high risk malignancy. The study used a fast track design with 1 patient per iTreg dose cohort (3.0 x 106/kg, 3.0 x 107/kg, 3.0 x 108/kg and 10.0 x 108/kg) along with CSA/MMF GVHD prophylaxis. An extension phase then occurred to total 10 patients at the best available dose, but using sirolimus/MMF as sirolimus is permissive of Treg expansion. HLA-identical sibling donors underwent 2 aphereses. On day -14, an unmobilized 15L apheresis was performed to collect cells for iTreg production. On day 0 (and +1 if needed), G-CSF mobilized 15L apheresis collected PBSCs. All patients received cyclophosphamide 50 mg/kg on day -6, fludarabine 30 mg/m2/day on days -6 to -2, and 200 cGy TBI as a single fraction on day -1. The iTregs were administered on day 0 at least 4 hours before the PBSC infusion.
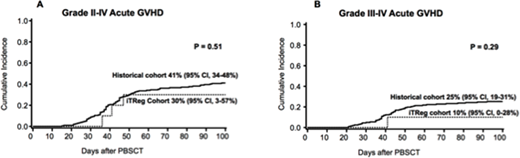
Results: Sixteen patients were enrolled. Two did not receive iTregs as inadequate numbers of cells were produced. 14 patients (7 male,7 female; median age 63 years) received iTregs. One patient each received 3.0 x 106/kg, 3.0 x 107/kg, 3.0 x 108/kg iTregs with a corresponding T effector:iTreg ratio of 86:1, 8:1 and 1:2. As a ratio of 1:1 was considered sufficient to suppress GVHD in mice, dose escalation was halted at 3.0 x 108/kg considering manufacturing costs despite no observed dose limiting toxicities (DLT). After 3 patients received 3.0 x 108/kg with CSA/MMF immunoprophylaxis with no DLTs, 2 patients received 3.0 x 108/kg iTregs using sirolimus/MMF. Both patients developed grade III aGVHD, resulting in suspension of the sirolimus/MMF arm. An additional 7 patients (for a total of 10) received 3.0 x 108/kg iTregs along with CSA/MMF. No severe infusional toxicities occurred in the 14 patients who received iTregs. All achieved neutrophil engraftment at a median of 7 days. Of 10 patients who received 3.0 x 108/kg iTregs using CSA/MMF, 2 developed grade II and 1 grade III aGVHD by day 100. Circulating Foxp3+iTregs were detected early after adoptive transfer, but were not detectable beyond day 28. Higher numbers of iTregs were detected at day 3 in patients who received 3.0 x 108/kg iTregs along with CSA/MMF versus 3.0 x 106/kg or 3.0 x 107/kg (21% +/-3% vs 9% +/- 3% of CD4 cells were Foxp3+CD25+). On day 7, lower numbers were seen in all patients and by day 28 only 3% of CD4+ cells were Foxp3+CD25 in all patients. In a contemporary institutional cohort of 203 adult patients with malignancies receiving the same RIC and GVHD prophylaxis, but without iTregs, the probabilities of grade II-IV aGVHD was 41% (95% CI, 34-48%) and grade III-IV GVHD was 25% (95% CI, 19-31%) suggesting iTreg administration may suppress GVHD to some extent in this small trial (Figure).
Conclusions: HLA-identical sibling donor iTregs were safely administered in the setting of HLA-identical sibling PBSCT. 3 x 108/kg iTreg/kg was the best tested dose to suppress GVHD with CSA/MMF immunoprophylaxis. Sirolimus/MMF was ineffective as GVHD prophylaxis in this iTreg clinical trial. Future studies should test the combination of iTregs and tTregs which synergistically induce tolerance in mice.
MacMillan:Angiocrine: Membership on an entity's Board of Directors or advisory committees; CSL Behring: Consultancy; Equillium: Consultancy. Brunstein:Gamidacell: Research Funding. Weisdorf:FATE: Consultancy; SL Behring: Consultancy; Seattle Genetics: Consultancy; Pharmacyclics: Consultancy; Equillium: Consultancy. Blazar:Kadmon Corporation, LLC: Consultancy, Research Funding. Wagner:Magenta Therapeutics: Consultancy, Research Funding; Novartis: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal