


Introduction: Daratumumab (DARA) is a human, CD38-targeted, IgG1κ monoclonal antibody approved as monotherapy in heavily pretreated relapsed/refractory multiple myeloma (RRMM) and in combination with standard-of-care regimens for transplant-ineligible NDMM and RRMM. The addition of DARA to standard-of-care regimens in phase 3 studies has consistently demonstrated a near doubling of complete response (CR) rates, tripling of minimal residual disease (MRD)-negativity rates, and reduction in the risk of disease progression or death by ≥44% in patients with transplant-ineligible NDMM or RRMM. In the primary analysis of the phase 3 MAIA study (median follow-up: 28.0 months), a significant progression-free survival (PFS) benefit (median not reached [NR] vs 31.9 months; hazard ratio [HR], 0.56; P<0.001) and a >3-fold increase in MRD-negativity rates (10-5 sensitivity threshold; 24.2% vs 7.3%; P<0.001) were observed for D-Rd vs Rd in patients with transplant-ineligible NDMM (Facon T, N Engl J Med 2019). Here, we report updated efficacy and safety findings from MAIA after 9 months of additional follow-up.
Methods: Patients with NDMM ineligible for high-dose chemotherapy and autologous stem cell transplantation due to age ≥65 years or comorbidities were randomly assigned (1:1) to receive Rd ± DARA. Stratification factors included International Staging System stage (ISS [I vs II vs III]), region (North America vs other), and age (<75 vs ≥75 years). All patients received 28-day cycles of Rd (R: 25 mg orally once daily on Days 1-21; d: 40 mg orally on Days 1, 8, 15 and 22). In the D-Rd arm, DARA (16 mg/kg intravenously) was given weekly for Cycles 1-2, bi-weekly for Cycles 3-6, and every 4 weeks thereafter. Patients were treated until disease progression or unacceptable toxicity in both treatment arms. The primary endpoint was PFS. Key secondary endpoints included overall response rate (ORR), MRD-negativity rate (10-5 sensitivity, clonoSEQ® version 2.0), and safety. PFS on the next line of therapy (PFS2), defined as the time from randomization to progression on the next line of therapy or death, was also measured.
Results: A total of 737 patients were randomized (D-Rd, N = 368; Rd, N = 369). Patient baseline characteristics were well balanced between the two treatment arms. Median (range) age was 73 (45-90) years, with 44% of patients ≥75 years of age. 27%, 43%, and 29% of all patients were ISS stage I, II, and III, respectively. Among 642 patients evaluable for FISH/karyotyping analysis, 86% had standard and 14% had high cytogenetic risk.
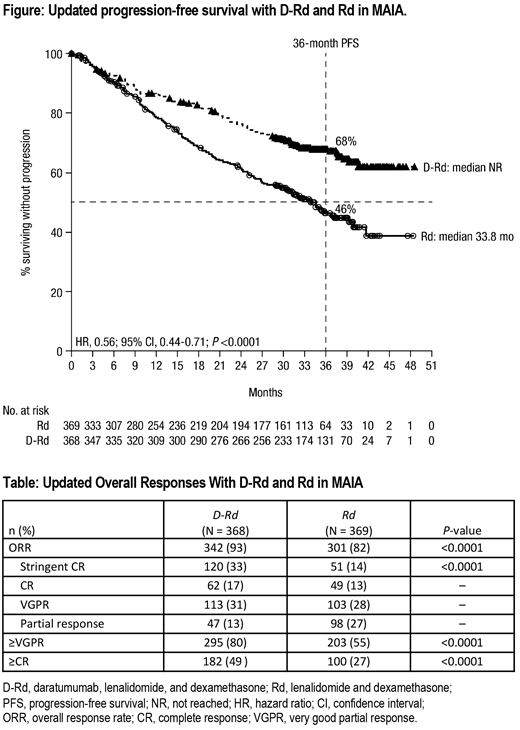
After a median follow-up of 36.4 months, median PFS was NR with D-Rd vs 33.8 months with Rd (HR, 0.56; 95% confidence interval [CI], 0.44-0.71; P<0.0001; Figure). The estimated 36-month PFS rate was 68% with D-Rd vs 46% with Rd. The PFS benefit of D-Rd vs Rd was observed in all prespecified subgroups, except for patients with impaired hepatic function. Adding DARA to Rd continued to result in deeper responses with higher rates of ≥CR and ≥very good partial response (VGPR; Table). Median duration of response among responders was NR with D-Rd vs 40.7 months with Rd. Median PFS2 was NR vs 47.3 months with D-Rd vs Rd, respectively (HR, 0.69; 95% CI, 0.53-0.91; P=0.0079); follow up is ongoing. 143 (39%) vs 233 (64%) patients with D-Rd vs Rd, respectively, have discontinued treatment. 85 (23%) patients with D-Rd vs 103 (28%) patients with Rd have discontinued the study due to death.
Grade 3/4 treatment-emergent adverse events (TEAEs; D-Rd/Rd) occurring in ≥10% of patients were neutropenia (51%/35%), lymphopenia (15%/11%), pneumonia (15%/9%), anemia (14%/21%), leukopenia (11%/6%), and hypokalemia (10%/10%); grade 3/4 infection rates were 36%/27%. The most common serious TEAE was pneumonia (14%/9%). 9% of patients in the D-Rd arm and 18% of patients in the Rd arm discontinued treatment due to TEAEs.
The complete updated data set will be presented at the meeting with additional efficacy endpoints, including MRD-negativity rate.
Conclusion: After longer follow up, the addition of DARA to Rd continues to demonstrate a significant PFS benefit and improved rates of deeper and more durable responses vs Rd alone in patients with transplant-ineligible NDMM. The longer follow-up also demonstrated a significant improvement in PFS2 favoring D-Rd, and no new safety concerns were observed. These results continue to support the use of D-Rd in the first line of treatment for transplant-ineligible patients with NDMM.
Bahlis:Janssen: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria; Celgene: Consultancy, Honoraria. Facon:Janssen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Takeda: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Sanofi: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees. Usmani:Amgen Array Biopharma, Bristol-Myers Squibb, Celgene, Janssen, Merck, Pharmacyclics, Sanofi, Takeda: Other: Research Grant; Amgen, Celgene, Janssen, Sanofi, Takeda: Speakers Bureau; Amgen, Bristol-Myers Squibb, Celgene, Janssen, Merck, SkylineDX, Takeda: Other: Consultant/Advisor. Kumar:Celgene: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Takeda: Research Funding. Plesner:Oncopeptides: Consultancy; Janssen: Consultancy, Research Funding; Takeda: Consultancy; AbbVie: Consultancy; Celgene: Consultancy; Genmab: Consultancy. Orlowski:Poseida Therapeutics, Inc.: Research Funding. Hulin:celgene: Consultancy, Honoraria; Janssen, AbbVie, Celgene, Amgen: Honoraria. Quach:Sanofi: Research Funding; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees, Research Funding; GSK: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding. Goldschmidt:ArtTempi: Honoraria; John Hopkins University: Other: Grants and/or provision of Investigational Medicinal Product; BMS: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Grants and/or provision of Investigational Medicinal Product, Research Funding; Novartis: Honoraria, Research Funding; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Grants and/or provision of Investigational Medicinal Product, Research Funding; Dietmar-Hopp-Foundation: Other: Grants and/or provision of Investigational Medicinal Product; Mundipharma: Research Funding; Adaptive Biotechnology: Membership on an entity's Board of Directors or advisory committees; MSD: Research Funding; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other, Research Funding; Amgen: Membership on an entity's Board of Directors or advisory committees, Other: Grants and/or provision of Investigational Medicinal Product, Research Funding; Sanofi: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Grants and/or provision of Investigational Medicinal Product, Research Funding; Molecular Partners: Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees, Research Funding; Chugai: Honoraria, Other: Grants and/or provision of Investigational Medicinal Product, Research Funding. O'Dwyer:GlycoMimetics Inc: Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; Onkimmune: Equity Ownership, Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Consultancy. Venner:Janssen: Honoraria; J&J: Research Funding; Amgen: Honoraria, Research Funding; Sanofi: Honoraria; Takeda: Honoraria; Celgene: Honoraria. Weisel:GSK: Honoraria; Takeda: Consultancy, Honoraria; Sanofi: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding; Juno: Consultancy; Celgene Corporation: Consultancy, Honoraria, Research Funding; Adaptive Biotech: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Honoraria; Amgen: Consultancy, Honoraria, Research Funding. Krevvata:Janssen: Employment. Pei:Janssen: Employment, Equity Ownership. Wang:Janssen: Employment. Van Rampelbergh:Janssen: Employment. Ukropec:Janssen: Employment, Equity Ownership. Uhlar:Janssen: Employment. Kobos:Janssen: Employment. Perrot:Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria; Amgen: Honoraria; Sanofi: Honoraria.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal