

Background
Granulocyte colony-stimulating factor (G-CSF) is the standard of care for mobilization of hematopoietic stem cells (HSCs). G-CSF requires 4-7 days of injections and often multiple aphereses to acquire sufficient CD34+ cells for transplant. The number of CD34+ HSCs mobilized can be variable and patients who fail to mobilize enough CD34+ cells are treated with the combination of G-CSF plus plerixafor. G-CSF use is associated with bone pain, nausea, headaches, fatigue, rare episodes of splenic rupture, and is contraindicated for patients with autoimmune and sickle cell disease. MGTA-145 (GroβT) is a CXCR2 agonist. MGTA-145, in combination with plerixafor, a CXCR4 inhibitor, has the potential to rapidly and reliably mobilize robust numbers of HSCs with a single dose and same-day apheresis for transplant that is free from G-CSF. MGTA-145 plus plerixafor work synergistically to rapidly mobilize HSCs in both mice and non-human primates (Hoggatt, Cell 2018; Goncalves, Blood 2018). Based on these data, Magenta initiated a Phase 1 dose-escalating study to evaluate the safety, PK and PD of MGTA-145 as a single agent and in combination with plerixafor.
Methods
This study consists of four parts. In Part A, healthy volunteers were dosed with MGTA-145 (0.0075 - 0.3 mg/kg) or placebo. In Part B, MGTA-145 dose levels from Part A were selected for use in combination with a clinically approved dose of plerixafor. In Part C, a single dose MGTA-145 plus plerixafor will be administered on day 1 and day 2. In Part D, MGTA-145 plus plerixafor will be administered followed by apheresis.
Results
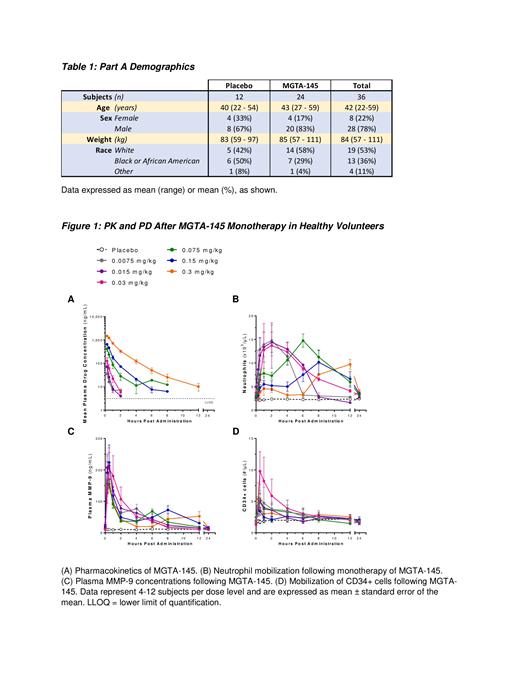
MGTA-145 monotherapy was well tolerated in all subjects dosed (Table 1) with no significant adverse events. Some subjects experienced mild (Grade 1) transient lower back pain that dissipated within minutes. In the ongoing study, the combination of MGTA-145 with plerixafor was well tolerated, with some donors experiencing Grade 1 and 2 gastrointestinal adverse events commonly observed with plerixafor alone.
Pharmacokinetic (PK) exposure and maximum plasma concentrations increased dose proportionally and were not affected by plerixafor (Fig 1A).
Monotherapy of MGTA-145 resulted in an immediate increase in neutrophils (Fig 1B) and release of plasma MMP-9 (Fig 1C). Neutrophil mobilization plateaued within 1-hour post MGTA-145 at doses greater than 0.03 mg/kg. This plateau was followed by a rebound of neutrophil mobilization which correlated with re-expression of CXCR2 and presence of MGTA-145 at pharmacologically active levels. Markers of neutrophil activation were relatively unchanged (<2-fold vs baseline). A rapid and statistically significant increase in CD34+ cells occurred @ 0.03 and 0.075 mg/kg of MGTA-145 (p < 0.01) relative to placebo with peak mobilization (Fig 1D) 30 minutes post MGTA-145 (7-fold above baseline @ 0.03 mg/kg).
To date, the combination of MGTA-145 plus plerixafor mobilized >20/µl CD34s in 92% (11/12) subjects compared to 50% (2/4) subjects receiving plerixafor alone. Preliminary data show that there was a significant increase in fold change relative to baseline in CD34+ cells (27x vs 13x) and phenotypic CD34+CD90+CD45RA- HSCs (38x vs 22x) mobilized by MGTA-145 with plerixafor. Mobilized CD34+ cells were detectable at 15 minutes with peak mobilization shifted 2 - 4 hours earlier for the combination vs plerixafor alone (4 - 6h vs 8 - 12h).
Detailed results of single dose administration of MGTA-145 and plerixafor given on one day as well as also on two sequential days will be presented along with fully characterized graft analysis post apheresis from subjects given MGTA-145 and plerixafor.
Conclusions
MGTA-145 is safe and well tolerated, as a monotherapy and in combination with plerixafor and induced rapid and robust mobilization of significant numbers of HSCs with a single dose in all subjects to date. Kinetics of CD34+ cell mobilization for the combination was immediate (4x increase vs no change for plerixafor alone @ 15 min) suggesting the mechanism of action of MGTA-145 plus plerixafor is different from plerixafor alone. Preliminary data demonstrate that MGTA-145 when combined with plerixafor results in a significant increase in CD34+ fold change relative to plerixafor alone. Magenta Therapeutics intends to develop MGTA-145 as a first line mobilization product for blood cancers, autoimmune and genetic diseases and plans a Phase 2 study in multiple myeloma and non-Hodgkin lymphoma in 2020.
DiPersio:Magenta Therapeutics: Equity Ownership; NeoImmune Tech: Research Funding; Cellworks Group, Inc.: Membership on an entity's Board of Directors or advisory committees; Karyopharm Therapeutics: Consultancy; Incyte: Consultancy, Research Funding; RiverVest Venture Partners Arch Oncology: Consultancy, Membership on an entity's Board of Directors or advisory committees; WUGEN: Equity Ownership, Patents & Royalties, Research Funding; Macrogenics: Research Funding, Speakers Bureau; Bioline Rx: Research Funding, Speakers Bureau; Celgene: Consultancy; Amphivena Therapeutics: Consultancy, Research Funding. Hoggatt:Magenta Therapeutics: Consultancy, Equity Ownership, Research Funding. Devine:Kiadis Pharma: Other: Protocol development (via institution); Bristol Myers: Other: Grant for monitoring support & travel support; Magenta Therapeutics: Other: Travel support for advisory board; My employer (National Marrow Donor Program) has equity interest in Magenta. Biernat:Medpace, Inc.: Employment. Howell:Magenta Therapeutics: Employment, Equity Ownership. Schmelmer:Magenta Therapeutics: Employment, Equity Ownership. Neale:Magenta Therapeutics: Employment, Equity Ownership. Boitano:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Cooke:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Goncalves:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Raffel:Magenta Therapeutics: Employment, Equity Ownership. Falahee:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Morrow:Magenta Therapeutics: Employment, Equity Ownership, Patents & Royalties. Davis:Magenta Therapeutics: Employment, Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal