


Introduction:
Clinical outcomes of acute myeloid leukemia (AML) in adolescents and young adults (AYA) are rarely reported as an isolated subgroup. Treatments vary little across age groups, and treatment intensity depends upon comorbid conditions and performance status. Optimal treatment strategies focused on disease behavior, biological factors, and the distinct needs of this subset of AML patients remain elusive. The purpose of this retrospective analysis is to determine the characteristics and outcomes of AYA AML patients treated at a specialized adult leukemia cancer center in comparison to older adults with AML (40-60 years).
Methods:
A retrospective analysis was performed on all patients treated at Princess Margaret Cancer Center from 2008-2018. Patients with acute promyelocytic leukemia were excluded. Clinical characteristics, treatment strategies, and survival outcomes were recorded for all patients.
Overall survival (OS) and disease-free survival (DFS) rates were calculated using the Kaplan-Meier product-limit method and the impact of covariates were assessed using the Log-rank test. Finally, we compared the outcomes of AYA patients treated at our centre between 2015-2018 with older patients.
Results:
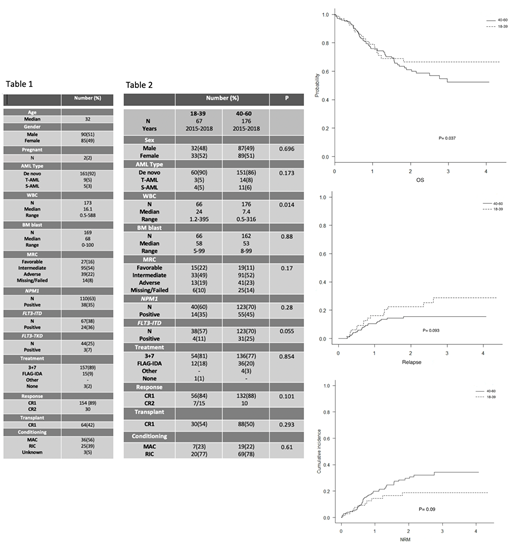
A total of 175 patients aged 18-39 were identified. Patient characteristics are shown in (Table 1). Cytogenetic were available in 163 patients. Based on MRC criteria, 27 (16%) were favorable risk, intermediate in 95 (54%), adverse in 39 (22%), and missing/failed in 14(8%). NPM1 status was available in 110 patients of whom 38 (35%) were positive. FLT3-ITD was available in 67 patients with 24 (36%) positive. Both mutations were present in 13 (54%) patients. There were no significant differences in terms of risk stratification based on cytogenetic and molecular markers based on age (18-29 vs.30-39) (P= 0.98).
Most patients 172 (98%) received induction, 157 (91%) with 3+7, and 15 (9%) with FLAG-IDA. Complete remission (CR) was achieved in 133 (77%) after first induction [120 (76%) after 3+7 and 11 (73%) after FLAG-IDA]. Induction related mortality was low (2%). Of the 39 who did not achieve CR, thirty-four patients received re-induction (13 FLAG-IDA, 16 NOVE-HiDAC, 5 others) with CR in 21 (62%). Overall, 154 (89.5%) achieved CR1. Sixty-four (42%) proceeded to hematopoietic stem cell transplantation (HSCT) in CR1.
59 (38%) patients relapsed in CR1 with 8 (12%) relapsing post HSCT. Fifty-five (5 post HSCT) patients received reinduction with 30 (51%) (2 after HSCT) achieving CR2. Fifteen patients received HSCT in CR2.
OS and DFS at 2 years were 62% (95% CI 0.53-0.69) and 50% (95% CI 0.41-0.57), respectively. Stratified by cytogenetic risk, OS was 81% for favorable risk, 61% for intermediate, and 50% for adverse risk (P=0.0001), respectively. DFS in these groups was 85%, 57%, and 46 % (P=0.0025), respectively. We further compared outcomes in the 18-29y and 30-39y age groups. The OS was 61.9% compared to 62.5% (P=0.91) and DFS of 52.1% compared to 47% (P=0.65) respectively.
On univariate analysis for OS and DFS, cytogenetic risk stratification was the only significant variable (P=0.0004 and P=0.0042).
We then compared the outcomes 67 sequential patients aged I8-39 treated from 2014-2018, with those of 176 sequential patients aged 40-60 treated during the same period (table 2). OS at 2 years was not statistically higher in the younger group compared to the older group (66.7% vs. 61.2%, P=0.372). While relapse rate was lower in older patients (15.5% vs. 22.6%, P=0.093), NRM was higher in older patients (29.7% vs. 18.8%,P=0.094).
Conclusion:
AYA pts. occupy a unique niche amongst AML as a whole. While treatment responses have improved in general, there may be potential for further gains in these patients. Increased tolerance for more intense treatment strategies as well as the incorporation of novel agents into standard treatment protocols may provide a means to optimize care in AYA patients. Finally, research is needed to elucidate biological mechanisms and predictors of disease behavior instead of arbitrary, age-stratified treatment schema.
McNamara:Novartis Pharmaceutical Canada Inc.: Consultancy. Schimmer:Jazz Pharmaceuticals: Consultancy; Medivir Pharmaceuticals: Research Funding; Novartis Pharmaceuticals: Consultancy; Otsuka Pharmaceuticals: Consultancy. Schuh:Astellas: Honoraria, Membership on an entity's Board of Directors or advisory committees; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Teva Canada Innovation: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Agios: Honoraria; Jazz: Honoraria, Membership on an entity's Board of Directors or advisory committees. Maze:Pfizer Inc: Consultancy; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees. Yee:Astellas: Membership on an entity's Board of Directors or advisory committees; Millennium: Research Funding; Takeda: Membership on an entity's Board of Directors or advisory committees; Astex: Research Funding; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Research Funding; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; MedImmune: Research Funding; Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Hoffman La Roche: Research Funding. Minden:Trillium Therapetuics: Other: licensing agreement. Gupta:Incyte: Honoraria, Research Funding; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Sierra Oncology: Honoraria, Membership on an entity's Board of Directors or advisory committees.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal