

Introduction
Acute myeloid leukemia (AML) is a very heterogeneous hematological malignancy characterized by the accumulation of myeloid blasts. Treatment options for unfit AML patients greater than 65 year of age are still limited and outcomes are dismal. The current standard of care for older AML patients are hypomethylating agents (HMA) or low dose Ara-C. However, even though inducing hematological remissions in up to 30 percent of the patients, responses are not durable and survival of these patients is only marginally prolonged. The poor durability is due to insufficient action on leukemia stem cells (LSC) which drive and maintain the disease and are resistance to therapy (Craddock et al, 2013 and DiNardo et al, 2019).
We described how aberrant CD70/CD27 signaling drives stemness of AML LSCs and identified CD70 as potential new target for the treatment of AML patients (Riether et al, 2017). In a recent Phase 1 clinical trial, treatment of older and unfit AML patients with the ADCC-enhanced humanized monoclonal anti CD70 antibody (mAb) cusatuzumab in combination with HMA demonstrated promising clinical activity and a favorable tolerability profile.
The BCL-2 antagonist, venetoclax, targets and eliminates LSCs by suppression of oxidative phosphorylation and demonstrated very promising activity in older AML patients in clinical phase I and II studies in combination with standard of care (Pollyea et al, 2018). However, even with novel agents such as venetoclax, there are still patients that become refractory or relapse. We hypothesized that combining venetoclax and cusatuzumab with distinct but complementary mechanisms of action could successfully eliminate LSCs.
Experimental design
To test this hypothesis, we performed a drug-combination study according to the Chou-Talalay method (Chou 2010) in CD70-expressing AML cell lines such as MOLM-13, MV4-11, and NOMO-1 cells in vitro. In addition, we tested the effect of the cusatuzumab/venetoclax and the cusatuzumab/venetoclax/HMA combination on colony formation and re-plating capacity of primary CD34+CD38- LSCs from newly diagnosed AML patients.
Results
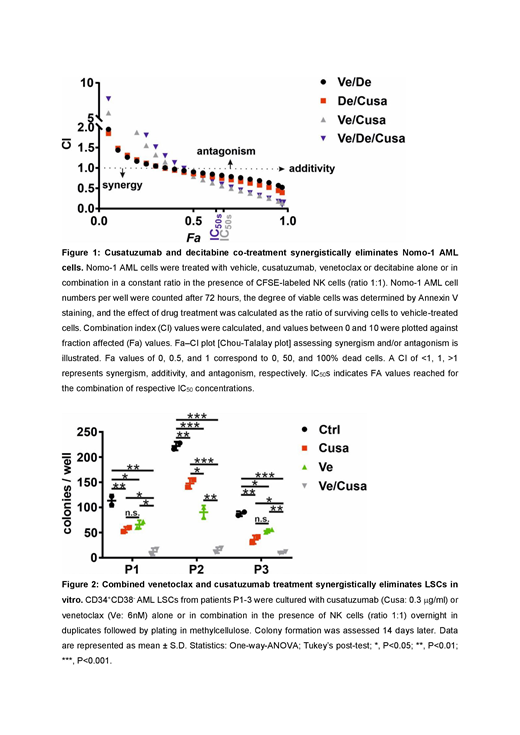
We first treated MOLM-13, MV4-11, and NOMO-1 AML cells with vehicle, cusatuzumab alone or in combination with venetoclax or decitabine in a constant ratio in the presence of CFSE-labeled NK cells (ratio 1:1). AML cell numbers were assessed 72 hours later. Cusatuzumab in combination with venetoclax or decitabine and NK cells synergistically eliminated CD70-expressing AML cells in a broad dose range (Figure 1).
To assess the effect of the cusatuzumab/venetoclax combination on primary human AML LSCs, we treated CD34+ CD38- LSCs with cusatuzumab or venetoclax monotherapy or in combination in the presence of NK cells and assessed colony formation. Cusatuzumab/venetoclax co-treatment was more efficacious than each monotherapy alone and strongly reduced LSCs and leukemia progenitors (Figure 2). To analyze the effect of the cusatuzumab/venetoclax treatment on LSC function in a more stringent way, we performed serial re-plating experiments in vitro. The impaired colony formation after combination treatment observed after the first plating was maintained during subsequent the re-plating, even though cusatuzumab and venetoclax were not present in the re-plating, indicating an effective reduction of LSCs. Mechanistically, we could show that treatment with venetoclax results in up-regulation of CD70 on LSCs, suggesting that venetoclax renders LSCs more susceptible to cytolytic killing with cusatuzumab.
In older AML patients, cusatuzumab and venetoclax each have demonstrated promising clinical activity in combination with HMA. We determined whether addition of HMA to the cusatuzumab/venetoclax co-treatment could more effectively eliminate LSCs. The triplet combination cusatuzumab/venetoclax/decitabine did not further reduce growth of AML cell lines in vitro (Figure 1) nor colony and re-plating capacity of human LSCs compared to the cusatuzumab/venetoclax co-treatment.
Conclusions
Overall, these results indicate that a combination of cusatuzumab with venetoclax eliminates LSCs synergistically and more efficiently than as a monotherapy. Tolerability and efficacy will be tested in mouse models using both primary AML and cell line xenografts. The results suggest that targeting LSCs by combining venetoclax and cusatuzumab treatments is a promising novel treatment strategy in AML.
Johnson:Janssen R&D: Employment. Drenberg:Janssen R&D: Employment. Syed:Janssen R&D: Employment. Moshir:Argenx: Employment, Equity Ownership. Hultberg:Argenx: Employment. Leupin:Argenx: Employment, Equity Ownership, Patents & Royalties. De Haard:Argenx: Employment, Equity Ownership, Patents & Royalties.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal