

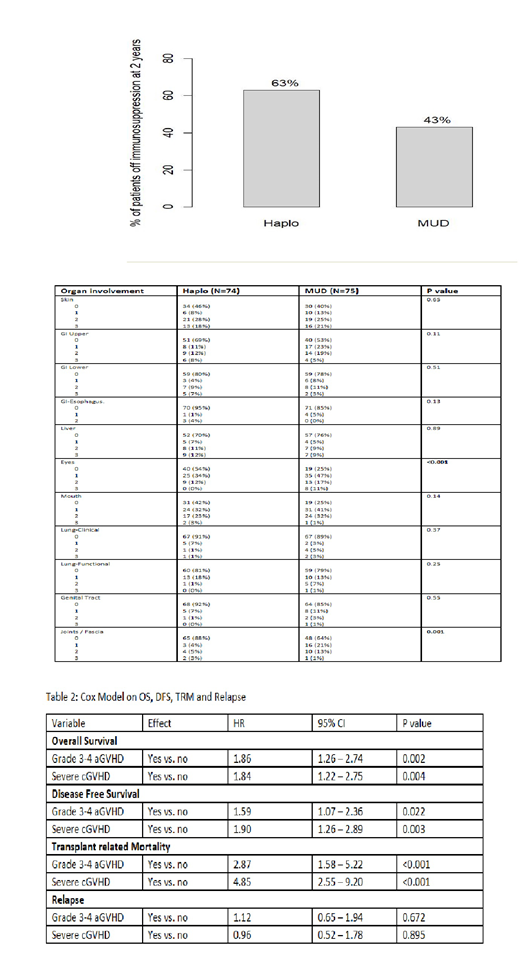
Unmanipulated T-cell replete HLA-mismatched haploidentical transplantation (haplo) with post-transplant cyclophosphamide (PTCY) is now widely used for patients lacking a suitably matched donor. The use of PTCY post haplo results in lower chronic GVHD rates compared to match unrelated donors (MUD) without PTCY. GVHD after PTCY in the haplo setting may have different presentation, response to treatment and impact on survival endpoints compared to a standard GVHD prophylaxis of calcineurin inhibitor plus MMF or methotrexate for MUD patients. To check for differences in GVHD presentation and response to treatment between MUD and haplo with PTCY, we assessed 394 consecutive patients who developed acute or chronic GVHD after receiving their first allogeneic transplantation (HCT) from a 10/10 HLA MUD (n=179) or a haplo (n=215) at our center between 2008 and 2017. Median follow up for survivors was 52.5 months. Our institution has prospectively documented onset, grading and therapy of patients with GVHD using a single dedicated practitioner since 2005. All haplo patients received standard GVHD prophylaxis of tacrolimus (days 5-180), MMF (stop day 35) and PTCY at 50mg/kg on days 3 and 4. Most commonly used GVHD prophylaxis for MUD patients were tacrolimus/methotrexate (68%) and tacrolimus/MMF (26%). MUD recipients were older (median age 56 vs 53 years, p=0.007), were more likely to be white (93% vs 58%, p<0.001), received mainly PBSC as graft source (76% vs 63%, p0.013) and had a higher HCT-comorbidity index (HCT-CI≥3, 64% vs 47%, p<0.001) compared to haplo recipients. The cumulative incidences for grade II-IV and III-IV aGVHD at day 180 post HCT were similar between both donor sources at 35% and 11% for haplo compared to 44% and 16% for MUD (p=NS). Haplo patients had lower cumulative incidence of mod-severe cGVHD at 22% versus 31% for MUD (p=0.026).The median times to onset of grade II-IV acute GVHD and moderate-severe chronic GVHD were: acute, 56 vs 49 days (p=0.19) and chronic 213 vs 280 days (p=0.011) for haplo versus MUD patients respectively. Among patients with grade II-IV acute GVHD, there was no significant difference in organ involvement between Haplo (n=101) and MUD (n=96) with skin being most commonly affected (74% haplo vs 71% MUD), Gut (70% haplo vs 69% MUD) and liver (14% haplo vs 17% MUD). For patients who developed chronic GVHD, organ involvement distribution is shown in table 1. Haplo patients had less involvement of the eyes (46% vs 75% for MUD, p<0.001) and of the joints/fascia (12% vs 36%, p=0.001). Among patients who developed grade II-IV acute GVHD, there was no difference in all-cause mortality (28% vs 19%, p=0.34) and being off immunosuppression at one 1 year (49% vs 51% p=0.80) between haplo and MUD recipients. Among patients who developed cGVHD, haplo recipients had similar all-cause mortality (22% vs 18%, p=0.89) but were more likely to be off immunosuppression at 2 years post HCT (63% vs 43% p=0.03) compared to MUD (figure 1). A cox model was conducted on survival and relapse endpoints where donor type was retained in all models. The fixed covariates tested in Cox models included age (<55, >=55), gender, race, diagnosis, regimen intensity, graft source (BM, PBSC), disease risk index (low/intermediate, high/very high), CIBMTR risk (low, intermediate, high), HCT-CI (0-2, >=3), CMV status, year of transplantation (2008-2012, 2013-2015, 2016-2017). The following variables were evaluated as time-dependent covariates in Cox models: all-grade cGVHD, moderate-severe cGVHD, severe cGVHD, grade 2-4 aGVHD, grade 3-4 aGVHD. Variables were selected if p values were less than 0.05. Developing grade 3-4aGVHD and severe chronic GVHD were both associated with worse OS, DFS and TRM (table 2). Both aGVHD and cGVHD were not significant factors for relapse. Our analysis reveals that compared to MUD, haplo transplant results in significantly lower incidence of moderate-severe chronic GVHD, faster cGVHD onset, different organ distribution and a higher chance of coming off immunosuppression. This data, added to prior publications from our center and others showing similar OS and DFS between MUD and haplo, enforces the notion that haplo transplant with PTCY is at least equivalent to MUD transplant. An ongoing BMTCTN 1702(CTRL-ALT-D) study will help answer assess this in a prospective fashion.
figure 1: Chronic GVHD patients who are Immunosuppression free at 2 years
Table 1: Organ Distribution of Chronic GVHD by Donor Type
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal