Key Points
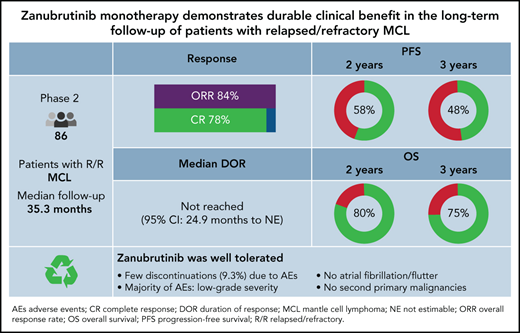
Zanubrutinib demonstrated deep and durable responses and a favorable safety profile in R/R MCL at median 35.3 months follow-up.
Zanubrutinib provided a high response rate (84% [78% CR]) and extended PFS (median 33.0 months) in patients with R/R MCL.

Abstract
Bruton tyrosine kinase (BTK) inhibitor is an established treatment for relapsed/refractory (R/R) mantle cell lymphoma (MCL). Zanubrutinib, a highly selective BTK inhibitor, is approved for patients with MCL who have received ≥1 prior therapy. We report the long-term safety and efficacy results from the multicenter, open-label, phase 2 registration trial of zanubrutinib. Patients (n = 86) received oral zanubrutinib 160 mg twice daily. The primary endpoint was the overall response rate (ORR), assessed per Lugano 2014. After a median follow-up of 35.3 months, the ORR was 83.7%, with 77.9% achieving complete response (CR); the median duration of response was not reached. Median progression-free survival (PFS) was 33.0 months (95% confidence interval [CI], 19.4-NE). The 36-month PFS and overall survival (OS) rates were 47.6% (95% CI, 36.2-58.1) and 74.8% (95% CI, 63.7-83.0), respectively. The safety profile was largely unchanged with extended follow-up. Most common (≥20%) all-grade adverse events (AEs) were neutrophil count decreased (46.5%), upper respiratory tract infection (38.4%), rash (36.0%), white blood cell count decreased (33.7%), and platelet count decreased (32.6%); most were grade 1/2 events. Most common (≥10%) grade ≥3 AEs were neutrophil count decreased (18.6%) and pneumonia (12.8%). Rates of infection, neutropenia, and bleeding were highest in the first 6 months of therapy and decreased thereafter. No cases of atrial fibrillation/flutter, grade ≥3 cardiac AEs, second primary malignancies, or tumor lysis syndrome were reported. After extended follow-up, zanubrutinib demonstrated durable responses and a favorable safety profile in R/R MCL. The trial is registered at ClinicalTrials.gov as NCT03206970.
Introduction
Mantle cell lymphoma (MCL) is an aggressive, incurable subtype of B-cell non-Hodgkin lymphoma; it has a relapsing and remitting clinical course and poor long-term prognosis.1,2 Even with recent advances in treatment, including the use of more intensive frontline therapies in younger, fitter patients, relapses in MCL are inevitable. Relapsed/refractory (R/R) MCL responds poorly to chemotherapy, and the expected survival is ∼1 to 3 years; as such, it is a major therapeutic challenge.3,4 Outcome is especially poor for patients with high-risk characteristics, including blastoid histology, TP53 mutation, refractory disease, and tumors with a high cell proliferation rate.5-8 While the optimal treatment approach to R/R MCL remains to be defined, Bruton tyrosine kinase (BTK) inhibitors have been validated as being among the most effective agents in this setting.2,9
Three BTK inhibitors are currently approved by the US Food and Drug Administration in R/R MCL: ibrutinib, acalabrutinib, and zanubrutinib.10-12 Ibrutinib, a first-in-class BTK inhibitor, demonstrated high activity in R/R MCL patients and changed the treatment paradigm for this population.13,14 Ibrutinib is associated with notable off-target toxicities, including diarrhea, rash, atrial fibrillation, bleeding, and arthralgias/myalgias that can limit its continuous use.15-18 Acalabrutinib, a second-generation BTK inhibitor, shows less off-target kinase inhibition relative to ibrutinib. Approval of acalabrutinib was based on a phase 2 study of 124 R/R MCL patients.19 With an extended follow-up of 38.1 months, overall response rate (ORR) was 81% (complete response [CR], 48%) and median progression-free survival (PFS) was 22 months. However, a high incidence of certain adverse events (AEs) was observed: headache (39% of patients) and grade 3/4 cardiac AEs (5% of patients).20
Zanubrutinib (BGB-3111) is a highly selective, potent, irreversible BTK inhibitor with favorable oral bioavailability. It was designed to achieve maximal exposure while minimizing inhibition of off-target kinases, such as epidermal growth factor receptor, interleukin–2-inducible kinase, and Src family kinases.21,22 Zanubrutinib demonstrated favorable safety and efficacy in 2 large-scale, phase 3, randomized studies in Waldenström macroglobulinemia (WM) (ASPEN study) and R/R chronic lymphocytic leukemia (CLL)/small lymphocytic lymphoma (SLL) (ALPINE study).23,24 In November 2019, zanubrutinib received accelerated approval in the United States as a treatment for MCL in adults with ≥1 prior therapy. This was based on a phase 2 study (BGB-3111-206) with 18.4 months follow-up.25 We report here longer-term follow-up (median, 35.3 months) of the safety and efficacy of zanubrutinib in this phase 2 trial, examining the durability of responses, long-term tolerability of zanubrutinib, and the molecular profile of nonresponding patients with R/R MCL.
Methods
Study design and patients
This single-arm, open-label, phase 2 study (ClinicalTrials.gov: NCT03206970) enrolled patients at 13 sites in China.25 Zanubrutinib was administered orally at a dose of 160 mg twice daily until progressive disease (PD), unacceptable toxicity, death, or withdrawal of consent.
Details of patient eligibility have been described previously.25 Key eligibility criteria were central pathologically confirmed MCL with measurable disease (≥1 but <5 prior lines of therapy), relapse or failure to achieve at least partial response (PR) to last regimen, age 18 to 75 years, and Eastern Cooperative Oncology Group performance status ≤2.
This study was conducted in accordance with sponsor procedures and in compliance with the ethical principles of the International Conference on Harmonization Guidelines for Good Clinical Practice and the Declaration of Helsinki and approved by local regulatory authorities. All patients provided written informed consent.
Efficacy and safety assessments
The primary endpoint was ORR, defined as either a PR or CR as assessed by the independent review committee (IRC), according to the Revised International Working Group Criteria for Malignant Lymphomas (the Lugano classification) and using a positron emission tomography (PET)-based assessment.26
Response evaluations were based on imaging assessment, clinical data, bone marrow (BM) biopsies, and gastrointestinal (GI) endoscopy, as assessed by the investigator and IRC. Response assessments, including PET scans and computed tomography (CT) with contrast, were performed every 12 weeks for 96 weeks and every 24 weeks thereafter until PD or withdrawal from the study. A BM biopsy was required to confirm a CR for patients with BM disease involvement at baseline. GI endoscopy was required to confirm a CR for patients with a documented history of GI involvement.
Secondary endpoints included investigator-assessed ORR, duration of response (DOR), time to response, PFS, and safety. Overall survival (OS) was an exploratory endpoint. AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA), version 23.0, and AEs of interest were categorized in accordance with predefined MedDRA search criteria based on the known toxicity profile of the BTK inhibitor class. Safety was assessed based on the frequency and severity of AEs graded according to the National Cancer Institute’s Common Toxicity Criteria for Adverse Events (NCI-CTCAE), version 4.03.
Mutational analysis
The mutation status of 175 hematological malignancy-related genes was assessed using a next-generation sequencing panel as previously described.25 All exons and partial introns of 175 genes were captured by probe hybridization, which can detect point mutation, insertion/deletion, and copy number alterations. The clinical significance of mutations was interpreted from publications, clinical guidelines, and a cancer mutation database. Mutations with clinical significance were used for downstream analysis. Fifty-six patients signed informed consent forms and provided sufficient formalin-fixed paraffin-embedded samples before zanubrutinib treatment for mutation assessment; 54 samples passed quality control process and obtained sequencing results. The median tumor cell percentage of the 54 samples was 95% (min, max: 40%, 98%).
Statistical analysis
Approximately 80 patients were planned for enrollment, primarily based on the intended level of precision of the estimated ORR. A sample of 80 patients provides 99% power to rule out a response rate of 40%, which is the minimal threshold for a clinically meaningful benefit if the true response rate is 70%, at a 1-sided α level of 0.025, using a binomial exact test. All results are presented through 8 September 2020 (study end date). Efficacy and safety analyses included patients who received ≥1 dose of zanubrutinib. An analysis of subgroups defined by baseline demographic and disease characteristics was performed for the proportion of patients achieving an objective response, CR, DOR, PFS, and OS. Time-to-event endpoints, including DOR, PFS, and OS, were analyzed using the Kaplan-Meier method with 95% confidence intervals (CIs).27,28 Event-free rates at selected time points (eg, 30 and 36 months) were estimated using the Kaplan-Meier method with 95% CIs.28,29 Patients were censored at the last adequate disease assessment (including imaging) for PFS and DOR before the initiation of subsequent anticancer therapy; those lacking either a baseline or ≥1 postbaseline response assessment were censored on the first day of study treatment.
Data sharing statement
On request, and subject to certain criteria, conditions, and exceptions, BeiGene will provide access to individual deidentified participant data from BeiGene-sponsored global interventional clinical studies conducted for medicines (1) for indications that have been approved or (2) in programs that have been terminated. Data requests may be submitted to DataDisclosure@beigene.com.
Results
Patients
Overall, 86 patients with R/R MCL were enrolled, all of whom received ≥1 dose of zanubrutinib and were evaluable for safety and efficacy. Patient baseline characteristics were published previously (supplemental Table 1). The median age was 61 years (range, 34-75), 77.9% were male, 83.7% had intermediate-/high-risk Combined MCL International Prognostic Index score (MIPI-b), and 14.0% had the blastoid variant of MCL. Most patients had advanced MCL (stage III/IV, 90.7%), 45.3% had BM involvement, and 70.9% had extranodal disease. Bulky disease (longest transverse diameter of a lesion [LDi]) >10 cm and >5 cm) was found in 8.1% and 43.0% of patients, respectively. The median number of prior lines of therapy was 2 (range, 1-4), and 52.3% of patients had refractory disease.
Exposure and patient disposition
After a median follow-up of 35.3 months (range, 0.3-41.6), 39 (45.3%) patients continued on treatment. The median treatment duration was 27.6 months (range, 0.2-41.6). For the 47 (54.7%) patients who discontinued treatment, reasons included PD (43%), AEs (9.3%), physician’s decision (1.2%), and withdrawal of consent after achieving CR (1 patient; 1.2%). Thirteen new patients who discontinued during the extended follow-up period were all due to PD. Twenty-one (24.4%) patients had died by data cutoff: 12 due to PD, 7 to AEs, and 2 for other reasons (due to unknown causes after receiving subsequent lines of therapy).
Efficacy
Response to zanubrutinib was maintained during this longer follow-up. The investigator-assessed ORR was 83.7% (95% CI, 74.2-90.8%), with a CR of 77.9% (Table 1). All responders achieved a response by the first efficacy assessment (12 weeks after the first dose of zanubrutinib), with a median time to response of 2.7 months (range, 2.5-3.0). After a median follow-up of 30.6 months from the initial response, median DOR was not reached (95% CI, 24.9 months-not estimable [NE]), and 57.3% (95% CI, 44.9-67.9%) of responders were estimated to be event-free (PD/death) at 30 months. Median PFS was 33.0 months (95% CI, 19.4-NE), and median OS was not reached. The estimated 24- and 36-month PFS event-free (PD/death) rates were 58.3% (95% CI, 46.9-68.2%) and 47.6% (95% CI, 36.2-58.1%), respectively (Figure 1A). The estimated 24- and 36-month OS rates were 80.4% (95% CI, 69.9-87.5%) and 74.8% (95% CI, 63.7-83.0%), respectively (Figure 1B). Categorical response attainment was associated with PFS and OS (Figure 1C-D). Median PFS was not reached in patients achieving CR (95% CI, 27.8-NE), whereas patients achieving PR or who were nonresponders (SD/PD) had a median PFS of 16.6 months (95% CI, 5.3-NE) and 2.6 months (95% CI, 0.8-2.9), respectively. A similar trend was observed for OS (Figure 1D). As of the data cutoff date, 37 patients had discontinued zanubrutinib treatment due to disease progression, 12 of which had died. The median OS among these 37 patients was 15.7 months (95% CI, 9.6-NE) with a median follow-up time of 11.3 months (range, 0.1-26.9).
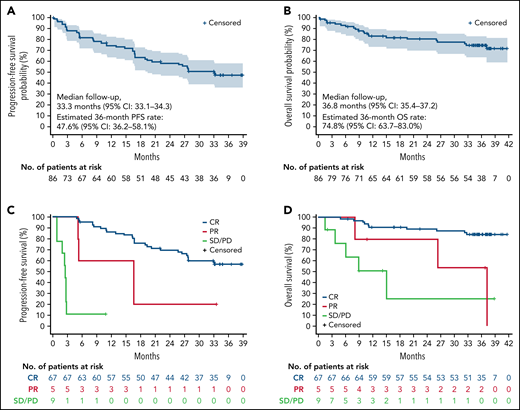
Kaplan-Meier curves of survival and response analyses. (A) PFS as determined by investigator assessment. Shaded area indicates 95% CI. (B) OS. Shaded area indicates 95% CI. (C) PFS by best overall response. (D) OS by best overall response. SD, stable disease.
Kaplan-Meier curves of survival and response analyses. (A) PFS as determined by investigator assessment. Shaded area indicates 95% CI. (B) OS. Shaded area indicates 95% CI. (C) PFS by best overall response. (D) OS by best overall response. SD, stable disease.
Subgroup analysis revealed that for response rates, there were no apparent differences across the subgroups analyzed, including poor-prognosis subgroups (supplemental Figure 1). ORR, DOR, PFS, and OS by specific subgroups with traditionally better or worse prognoses are summarized in Table 2 and supplemental Table 2. DOR and PFS were similar in patients with or without blastoid histology, bulky disease, or refractory disease. The median DOR and PFS were 30.2 months and 25.0 months in patients with blastoid histology, similar to patients with classic histology (median DOR, 30.6 months; PFS, 27.8 months) (supplemental Figure 2). However, prolonged DOR and PFS were observed in patients with low-/intermediate-risk MIPI-b, lower Ki67 index (≤30%), fewer prior lines of therapy, and TP53 wild type (WT) (Table 2; supplemental Table 2). Of the 54 patients with known TP53 mutation status, 15 (27.8%) had mutated TP53. In patients with mutated and WT TP53, respectively, median PFS was 14.7 months (95% CI, 2.9-NE) and not reached (95% CI, 19.4-NE), median OS was 37.1 months (95% CI, 4.9-NE) and not reached (95% CI, NE-NE) (supplemental Figure 3), and the overall response was similar (80.0% [95% CI, 51.9-95.7%] and 89.7% [95% CI, 75.8-97.1%]) (Table 2).
Safety
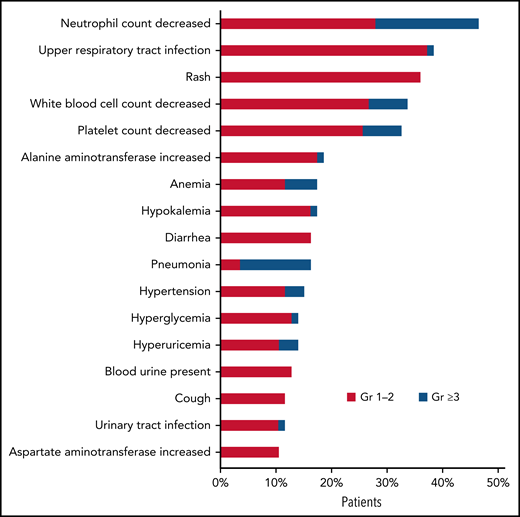
The safety profile with a median 35.3 months follow-up was largely unchanged from that in the previously reported 18.4 months follow-up. The most common treatment-emergent AEs (TEAEs), regardless of causality, in ≥20% of patients were neutrophil count decreased (46.5%), upper respiratory tract infection (38.4%), rash (36.0%), white blood cell count decreased (33.7%), and platelet count decreased (32.6%); most were grade 1/2 events. Grade ≥3 TEAEs were reported in 50.0% of patients and were most commonly (≥5%) neutrophil count decreased (18.6%), pneumonia (12.8%), platelet count decreased and white blood cell count decreased (7.0% each), and anemia (5.8%) (Figure 2).
Most AEs occurred during early-stage zanubrutinib treatment, and no new safety signals were observed after extended follow-up. The overall frequency of any grade or grade ≥3 AE of interest decreased over time on zanubrutinib therapy (Table 3). Most occurrences of bleeding, infection, and cytopenia were reported early in the treatment course, generally within 6 months of treatment (Table 3).
Infections were the most common category of AE of interest, with 65.1% of patients reporting ≥1 infection (supplemental Table 3). Upper respiratory tract infection was the most frequent (38.4%), followed by pneumonia (16.3%) and urinary tract infection (11.6%). Grade ≥3 infections were reported in 16 (18.6%) patients. Among the patients who reported infection, fungal pneumonia was suspected in 3 patients; it did not occur within 30 days of neutropenia in any of these patients. Bleeding events were reported in 36.0% of patients. Most were grade 1 or 2 bleeds involving mucous membranes and skin. Major hemorrhage was reported in 3 (3.5%) patients (1 with cerebral hemorrhage; 2 with GI hemorrhage); these were previously reported in detail, and no new cases occurred during the extended follow-up. All-grade neutropenia occurred in 50% of patients, with grade ≥3 neutropenia reported in 19.8%. All-grade and grade ≥3 neutropenia decreased over time, with no grade ≥3 neutropenia occurring after 18 months of treatment (Table 3). No patient required study drug discontinuation for neutropenia, but 3 patients (2 with neutrophil count decreased; 1 with febrile neutropenia) required treatment interruption. No cases of atrial fibrillation/flutter, grade ≥3 cardiac AEs, second primary malignancies, or tumor lysis syndrome were reported throughout this study.
No new deaths due to AEs occurred during the longer follow-up period. A total of 21 (24.4%) patients died, 8 within 30 days of the last study treatment (6 from complications of AEs; 2 from PD). As reported previously,25 AEs leading to death included 1 case each of traffic accident, left occipital lobe hemorrhage, and pneumonia, and 3 deaths were due to unknown causes (1 of which occurred after the patient began new anticancer therapy). Of the 13 deaths occurring >30 days after the last dose of the study drug, 10 were due to PD, 1 was due to worsening of a TEAE of fungal pneumonia, and 2 were for unknown causes after the patients received subsequent lines of therapy. Detailed information on AE-related deaths is provided in supplemental Table 4.
Mutation biomarker analysis
To explore the association between mutations and zanubrutinib response, the mutational status of 175 hematological malignancy-related genes was assessed in 54 patients. Of the 54 samples, 6 (11%) samples were collected at initial diagnosis; 35 (65%) were collected just before zanubrutinib and after the last line of treatment; and 11 (20%) were collected after initial treatment and before the last line of treatment before zanubrutinib. The sample collection date for 2 samples was unavailable.
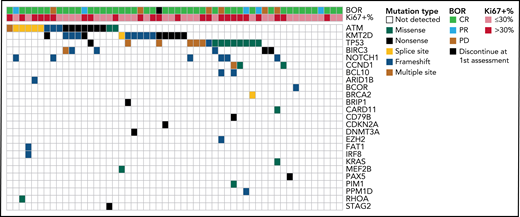
Consistent with other studies,30 most of the mutations were found in the cell cycle (TP53, CCND1, PPM1D, CDKN2A), epigenetic (KMT2D, ARID1B, DNMT3A, EZH2), DNA repair (BRCA2, BRIP1, ATM), B-cell receptor/NF-κB pathway (CD79B, BIRC3, CARD11, BCL10), and NOTCH pathway (NOTCH1) genes (Figure 3). Mutations in NF-κB pathway genes, including BIRC3, CARD11, and BCL10, were exclusive, a pattern that was also observed in ATM and TP53. Among the 54 patients, 6 had PD as the best overall response (BOR), 47 achieved CR or PR as BOR, and 1 discontinued zanubrutinib before the first response assessment. PD patients had higher mutation rates vs CR or PR patients: NOTCH1, 50.0% (3/6) vs 6.4% (3/47); BCL10/CARD11, 33.3% (2/6) vs 2.1% (1/47); and TP53, 50.0% (3/6) vs 25.5% (12/47). NOTCH1 and BCL10/CARD11 mutations tended to be associated with lower ORR and shorter PFS (Table 4).
Discussion
In this report of extended follow-up, we demonstrated the continued efficacy and favorable safety profile of single-agent zanubrutinib in patients with R/R MCL. After a median follow-up of 35.3 months, the BOR was maintained, with an ORR of 83.7% (CR, 77.9%), as assessed by the investigator. ORR was consistent with the previously reported IRC assessment (ORR, 83.7%).25 A similar ORR (84.4%) and median time to response (2.7 months) were demonstrated in a zanubrutinib first-in-human study (BGB-3111-AU003) of 37 R/R MCL patients,31 thus confirming the efficacy profile of zanubrutinib in this disease setting.
Responses in the present study were durable, as well as high and deep. Median DOR was not reached, median PFS was 33.0 months, and the 36-month OS rate was 74.8%. Pooled data from 3 single-agent studies of ibrutinib in R/R MCL (PCYC-1104, RAY, and SPARK; n = 370), with a median number of prior lines of therapy of 2 (1-9), showed an ORR of 70% (CR, 27%) at 3.5 years follow-up. Median DOR, PFS, and OS were 21.8, 12.5, and 26.7 months, respectively.32 In the acalabrutinib pivotal phase 2 study (ACE-LY-004; n = 134), with a median number of prior lines of therapy of 2 (1-5), an ORR of 81% (CR, 48%) was observed at 38.1 months follow-up. Median DOR and PFS were 28.6 and 22.0 months, respectively, and the estimated 36-month OS rate was 60.5%.20 It is important to highlight that, unlike the present study and the acalabrutinib study, which were based on regular PET assessment, the ibrutinib studies used CT-based response assessment. Nevertheless, the impact of the lack of PET is almost negligible when comparing survival outcomes.
As discussed in the previous report,25 the differences in baseline demographic and disease characteristics, although generally comparable, may limit the comparability of efficacy outcomes across studies. Most prognostic variables (eg, presence of bulky disease, blastoid histology, refractory disease, extranodal involvement, and proportion with MIPI scores) were similar, but there was a notable difference in median age.19,20,32 In the present study, the median age was 61 years, which is younger than in the ibrutinib (67.5 years) and acalabrutinib (68 years) studies. However, an interesting finding is that the efficacy did not differ by age subgroup. In the present study, although inferior ORR and CR rates were observed in older patients, numerically superior PFS and OS were demonstrated for these patients.
It is noteworthy that a consistent finding from these BTK inhibitor analyses is that DOR, PFS, and OS are proportionate to the depth of response. Patients achieving a CR showed prolonged PFS and OS compared with those with PR or nonresponders.6,20 In the present study, of patients achieving CR, 56.5% were progression-/death-free, and 84.3% were alive at 36 months. The high and deep responses observed in this study have been translated into meaningful long-term survival and may be attributable to the selectivity and favorable pharmacokinetic profile of zanubrutinib. Achieving complete and sustained BTK occupancy in both peripheral blood mononuclear cells and lymph node biopsy tissues is hypothesized to provide the high, deep, and durable responses seen in patients receiving zanubrutinib. This may be attributed to the observation of similar efficacy in patients with or without bulky disease (LDi >10 cm or >5 cm), as generally similar ORR, CR rate, PFS, and OS were achieved. In contrast, CR rate, PFS, and OS were lower for patients with bulky disease treated with ibrutinib compared with the patients without bulky disease.7
TP53 mutation and blastoid histology subtypes are critical prognostic factors in MCL. They are strongly associated with inferior survival, and the outcome has not obviously been shown to improve with the new agent ibrutinib.8,32,33 Although a less favorable outcome was observed compared with TP53 WT patients, patients with TP53 mutation in the present study who achieved an ORR of 80.0%, median PFS of 14.7 months, and 36-month OS of 57.1% appear to be substantially better than those reported and provide an encouraging treatment option for patients with this particularly dismal prognosis. Recognizing the limitation of the small sample size in this study, it is nevertheless noteworthy that the benefit seen with zanubrutinib treatment was in patients with blastoid histology (who achieved similar DOR and PFS to those with classic histology). As expected, patients with low-/intermediate-risk MIPI-b score and low Ki67 percentage (≤30%) demonstrated a longer PFS and OS. These data highlight the unmet need in patients with a highly proliferative disease whose outcomes may be improved by the addition of other active agents to a BTK inhibitor; however, further study is needed to determine effective combination therapy approaches.2,34,35 In preclinical studies, zanubrutinib was at least 10-fold weaker than ibrutinib in inhibiting rituximab-induced antibody-dependent cell-mediated cytotoxicity, and it demonstrated good combination activity with rituximab in preclinical xenograft models.21,36,37 Because of these encouraging results, we initiated a frontline phase 3 trial (NCT04002297) in MCL comparing zanubrutinib plus rituximab, followed by zanubrutinib monotherapy, vs bendamustine plus rituximab, followed by observation, in ∼500 adult patients.38
Truncating or frameshift mutations on the NOTCH1 PEST domain were found in 12% of MCL patients, a pattern and frequency that have similarly been found in CLL patients.39 Mutations on the NOTCH1 PEST domain can inhibit its proteasome degradation and constitutively activate the NOTCH pathway,40 thereby contributing to B-CLL cell survival and resistance to apoptosis.41NOTCH1 mutations are not only associated with worse PFS in CLL patients receiving ibrutinib therapy,42 they are also linked to worse prognosis outcomes in MCL patients on chemoimmunotherapy.39 In the current study, NOTCH1 mutations were discovered in 11.1% (6/54) of patients with R/R MCL; all were frameshift mutations and localized on the PEST domain. In 50% (3/6) of NOTCH1-mutant patients, there was no response to zanubrutinib, and the BOR was PD. The MCL3001 (RAY) study, comparing ibrutinib and temsirolimus in R/R MCL, showed that 50% (1/2) and 0% (0/3) of NOTCH1-mutant MCL patients had durable responses to ibrutinib and temsirolimus, respectively.43 Ibrutinib and venetoclax combination therapy is recommended by the National Comprehensive Cancer Network for R/R MCL patients, but NOTCH1-mutant R/R MCL patients still do not appear to receive additional benefit from this combination regimen. Among 24 enrolled MCL patients receiving ibrutinib and venetoclax combination, NOTCH1 PEST domain mutations were detected in 12.5% (3/24) of patients, all of whom had PD and did not respond to therapy.33 These data indicate that NOTCH1 mutation is a risk factor in MCL patients, and the clinical benefit of new treatment regimens for this population should be further assessed. Constitutive activation of the NF-kB pathway occurred in different B-cell lymphoid malignancies and regulated antiapoptotic and proproliferative gene expression. Aberrant NF-kB activation was associated with poor clinical outcome.44 In the B-cell receptor signaling pathway, BTK-dependent NF-kB activation is regulated by the CARD11–BCL10–MALT1 (CBM) complex, including CARD11, BCL10, and MALT1 proteins, and active mutations in the CBM complex have been reported in WM, follicular lymphoma, primary central nervous system lymphoma, and MCL, and are associated with poor response to ibrutinib.43,45-47 In the present study, 3 patients had CARD11 or BCL10 active mutations, 2 of whom failed to respond to zanubrutinib (BOR of PD). This indicates that, as a downstream effector of the BTK signal, NF-kB activation contributes to the poor response to BTK inhibitors.
Two recent phase 3, randomized, head-to-head studies in patients with WM and R/R CLL/SLL demonstrated advantages of zanubrutinib vs ibrutinib in safety and tolerability.23,24 A consistent safety profile of zanubrutinib was observed in the present study; the long-term favorable tolerability of zanubrutinib was further established in this study with extended follow-up. The incidence of AEs decreased over time, and no new safety signals were observed. The most common AE and grade ≥3 AE observed in the present study were both neutrophil count decreased (46.5% and 18.6%, respectively), which is believed to be related to the on-target inhibition of BTK in neutrophil precursors. The incidence of neutropenia decreased after the first year, and no grade ≥3 neutropenia occurred after 18 months. In the extended follow-up period, no new patient had grade ≥3 AEs of hypertension or major hemorrhage. Importantly, no cases of atrial fibrillation/flutter, grade ≥3 cardiac AEs, grade ≥3 diarrhea, second primary malignancies, or tumor lysis syndrome were reported throughout this study. AEs leading to treatment modification were infrequent in the current study, and no treatment discontinuations or dose reductions occurred due to AEs in the extended long-term follow-up. As demonstrated in the retrospective analyses of ibrutinib treatment intensities in both CLL/SLL48,49 and WM,50 the ability to maintain sustained BTK inhibition through adherence to the prescribed treatment regimen appears to be critical for optimal disease control in patients with B-cell neoplasms. Adherence to the prescribed treatment regimen can be further impacted by lower acuity AEs that nevertheless impact patient quality of life. Ibrutinib and acalabrutinib are associated with arthralgias and myalgias in 15% to 20% of patients, and diarrhea in 30% to 50% (grade ≥3, 3-5%); headache is seen in up to 40% of patients receiving acalabrutinib.10,11,51 These toxicities were rarely observed in the current study of zanubrutinib, which potentially contributed to the overall high level of adherence to treatment and possibly translated into a favorable efficacy profile.
In conclusion, this phase 2 study in patients with R/R MCL with extended 35.3-month follow-up data continued to demonstrate a favorable benefit–risk profile of zanubrutinib monotherapy in R/R MCL patients. Approximately 50% of patients remain progression-free at 36 months.
Acknowledgments
The authors thank the patients who participated in the study, their supporters, and the investigators and clinical research staff from the study centers.
Medical writing and editorial assistance were funded by BeiGene and were provided, under the direction of the authors, by Richard Delarue of BeiGene, and by Ify Sargeant of Twist Medical. This work was supported by research funding from BeiGene Ltd., Beijing, China, and BeiGene USA, Inc., San Mateo, CA.
Authorship
Contribution: Y.S., K.Z., D.Z., H.G., L.Z., J.H., W.N., Y.Y., B.W., and J. Zhu contributed to the conception and design of the study; K.Z., D.Z., H.G., L.Z., J.H., Y.Y., B.W., and J. Zhu provided methodology development; Y.S., K.Z., D.Z., J. Zhou, J.H., H.Y., H.Z., J. Ji, W.X., J. Jin, F.L., R.F., S.G., H.G., L.Z., Y.Y., B.W., and J. Zhu acquired data (provided animals, acquired and managed patients, provided facilities, etc); Y.S., K.Z., D.Z., F.L., H.G., L.Z., R.F., J.H., W.N., P.K., Y.Y., B.W., and J. Zhu provided analysis and interpretation of data (eg, statistical analysis, biostatistics, computational analysis); Y.S., K.Z., D.Z., J.H., H.Y., H.Z., J. Ji, J. Jin, F.L., S.G., H.G., L.Z., R.F., J.H., W.N., P.K., Y.Y., B.W., and J. Zhu wrote, reviewed, and/or revised the manuscript; Y.S., K.Z., D.Z., J. Jin, H.G., L.Z., J.H., Y.Y., B.W., and J. Zhu provided administrative, technical, or material support (ie, reporting or organizing data, constructing databases); and Y.S., K.Z., D.Z., H.Y., S.G., H.G., L. Zhou, J.H., W.N., and J. Zhu supervised the study.
Conflict-of-interest disclosure: J.H., W.N., H.G., L.Z., P.K., Y.Y., and B.W. are employees/paid consultants for BeiGene. All other authors declare no competing financial interests.
Correspondence: Jun Zhu, Peking University Cancer Hospital & Institute, No. 52, Fucheng Rd, Haidian District, Beijing 100142, China; e-mail: zhu-jun2017@outlook.com.
There is a Blood Commentary on this article in this issue.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.