


Introduction
Venetoclax (VEN), a potent BCL2 inhibitor, demonstrated favorable outcomes combined with hypomethylating agents and low dose cytarabine (AraC) in elderly patients (pts) newly diagnosed (ND) with acute myeloid leukemia (AML). In order to improve both remission rates and survival in fit AML pts, we evaluated the combination of VEN with FLAG-IDA regimen in fit pts with ND or relapsed/refractory (R/R) AML.
Objectives
This phase (Ph) Ib/II single center clinical trial has dual primary objectives: (1) Safety and tolerability of the combination for pts with R/R AML (Ph Ib), and (2) Overall response rate (ORR) by modified IWG AML criteria in pts ND or R/R AML (Ph II). Secondary analyses include duration of response (DOR) and overall survival (OS).
Methods
Eligibility includes medically fit, ND or R/R AML pts of any age with adequate organ function, PS ≤ 2, and WBC < 25x109/L. Only R/R AML pts were eligible for Ph Ib dose escalation. Pts receive FLAG-IDA induction/consolidation (ind/cons), with VEN orally daily. The original FLAG-IDA ind consisted of fludarabine 30 mg/m2 IV D2-6, AraC 2 g/m2 IV D2-6, idarubicin 6 mg/m2 IV D4-6 (8 mg/m2 IV D4-6 for ND pts), and filgrastim 5 mcg/kg daily D1-7 (or pegfilgrastim 6 mg after day 5 to replace remaining injections).
The 3+3 algorithm was applied for dose escalation. The first cohort (dose -1, n=8) received FLAG-IDA with VEN 200 mg on days 1-21 of ind, incorporating a 2-day VEN dose ramp up. After the observation of gram negative bacteremia and/or sepsis in 5 of 6 pts during cycle 1 nadir, an amended dose level -1 ind was designed with reduced AraC 1.5 g/m², with VEN 200 mg on D1-14 and dose level 0 with VEN 400mg on D1-14. After completion of ind/cons, single agent VEN at 400 mg continuously is provided as maintenance for pts not proceeding to alloSCT. The data cutoff was 6.10.2019.
Results
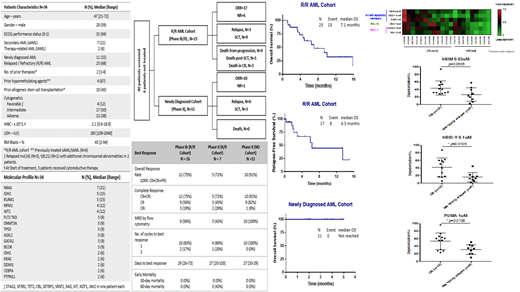
At data cutoff, 34 pts with a median age of 47 yrs (range, 21-72) have been enrolled: 16 pts in the Ph Ib, and 18 pts in Ph II (11 in ND, and 7 in R/R cohort). 23 pts had R/R AML with a median of 2 (range, 1-4) prior therapies, and 10 (43%) pts had received prior alloSCT. Additional demographics including molecular profile at study enrollment are provided in Table 1.
The median number of cycles received is 2 (range, 1-4). VEN 400 mg on D1-14 was considered safe for Ph II dose expansion. Serious adverse events regardless of causality were infections (n=26), bacteremia (n=12), sepsis (n=5), hypotension (n=4) and typhlitis (n=3). No tumor lysis syndrome was identified. 30-day mortality was 0%, 60-day mortality was 0% in ND cohort and 13% in R/R cohort (2 pts died from progression and 1 pt from fungal pneumonia).
All enrolled pts were evaluable for response. Of 23 R/R pts, 17 pts (74%) achieved a best response of CR/CRi (12 CR, 5 CRi: 3 CRh + 2 CRp). 12 (52%) pts attained MRD negative status by flow cytometry. 15 pts attained a best response after one cycle, and two attained blast reduction after cycle 1 followed by CR after re-induction. Among responders, 9 pts proceeded to alloSCT, 2 remain on study, 3 pts relapsed, and 3 pts died in CR at 1.7, 3.4 and 4.6 months on treatment. Median time to ANC recovery > 500/ul and platelet recovery > 50K in responders was 27 days (range, 20-90) and 33 days (range, 20-54) respectively. With a median follow-up of 5 months, median DOR is not reached and OS is 7.1 months. Median OS for pts in salvage 1, 2, and ≥ 3 is 9.4, 10, and 4.9 months, respectively.
Of 11 ND pts, 10 pts (91%) achieved ORR (9 CR, 1 CRh) and all 10 pts became MRD negative by flow cytometry: 3 pts proceeded to alloSCT, and 7 pts remain on active treatment. Median time to ANC and platelet recovery with induction was 23 days (range, 19-31) and 25 days (range, 18-31) respectively. Both DOR and OS are not estimable.
Of interest, responding pts demonstrated higher apoptosis priming, as shown by depolarization in response to Bid, PUMA and Bim peptides by BH3 profiling (Fig 1).
Conclusions
FLAG-IDA with VEN demonstrates notable activity in both R/R and ND medically fit pts. Improved safety and tolerability without decreasing efficacy was achieved by decreasing AraC to 1.5 g/m2, and administering VEN for 14 days in ind, and 7 days in cons cycles. Neither prolonged cytopenias nor early mortality were observed. Ph II portion for R/R and ND pts is ongoing. Correlative studies with genomic annotation, CyTOF analysis and BH3 profiling are being analyzed, with higher apoptosis priming identified in responding pts. Longer follow-up is necessary to establish long term survival benefit.
Konopleva:Stemline Therapeutics: Consultancy, Honoraria, Research Funding; Kisoji: Consultancy, Honoraria; Reata Pharmaceuticals: Equity Ownership, Patents & Royalties; Calithera: Research Funding; Ablynx: Research Funding; Astra Zeneca: Research Funding; Agios: Research Funding; Forty-Seven: Consultancy, Honoraria; Eli Lilly: Research Funding; AbbVie: Consultancy, Honoraria, Research Funding; Cellectis: Research Funding; Amgen: Consultancy, Honoraria; F. Hoffman La-Roche: Consultancy, Honoraria, Research Funding; Genentech: Honoraria, Research Funding; Ascentage: Research Funding. Kadia:Jazz: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Research Funding; Pfizer: Membership on an entity's Board of Directors or advisory committees, Research Funding; Bioline RX: Research Funding; Pharmacyclics: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; Genentech: Membership on an entity's Board of Directors or advisory committees; BMS: Research Funding; Amgen: Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Consultancy, Research Funding. Takahashi:Symbio Pharmaceuticals: Consultancy. Jabbour:Takeda: Consultancy, Research Funding; BMS: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Amgen: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Cyclacel LTD: Research Funding. Garcia-Manero:Helsinn: Research Funding; Novartis: Research Funding; AbbVie: Research Funding; Celgene: Consultancy, Research Funding; Astex: Consultancy, Research Funding; Onconova: Research Funding; H3 Biomedicine: Research Funding; Merck: Research Funding; Amphivena: Consultancy, Research Funding. Ravandi:Xencor: Consultancy, Research Funding; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Selvita: Research Funding; Cyclacel LTD: Research Funding; Macrogenix: Consultancy, Research Funding; Menarini Ricerche: Research Funding. Cortes:BMS: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Daiichi: Consultancy, Research Funding; Astellas: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Biopath: Consultancy; BiolineRx: Consultancy, Research Funding; Merus: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Jazz: Consultancy, Research Funding. Kantarjian:Pfizer: Honoraria, Research Funding; Immunogen: Research Funding; BMS: Research Funding; Cyclacel: Research Funding; Daiichi-Sankyo: Research Funding; Agios: Honoraria, Research Funding; AbbVie: Honoraria, Research Funding; Novartis: Research Funding; Ariad: Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria; Jazz Pharma: Research Funding; Amgen: Honoraria, Research Funding; Astex: Research Funding. DiNardo:celgene: Consultancy, Honoraria; daiichi sankyo: Honoraria; notable labs: Membership on an entity's Board of Directors or advisory committees; agios: Consultancy, Honoraria; syros: Honoraria; abbvie: Consultancy, Honoraria; medimmune: Honoraria; jazz: Honoraria.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal