

Introduction
Immunomodulatory agents (IMiD's) are associated with an increased risk of venous thromboembolism (VTE), particularly when combined with high dose steroids. Studies evaluating the use of lenalidomide-bortezomib-dexamethasone (RVD) and carfilzomib-lenalidomide-dexamethasone (KRD) in the frontline setting for multiple myeloma (MM) have reported a 6% and 24% incidence of thrombosis, respectively, despite primary thrombotic prophylaxis with aspirin (ASA) (Richardson, et al. Blood. 2010; Korde, et al. JAMA Oncol 2015). Recent data, including the Hokusai VTE Cancer Trial, have suggested that safety and efficacy of direct oral anticoagulants (DOACs) are preserved in the setting of treatment of solid malignancy-associated thrombosis (Raskob, et al. N Engl J Med. 2018; Mantha, et al. J Thromb Thrombolysis. 2017). Despite this data, there is limited experience and use of DOACs in prevention of thromboses in the setting of hematologic malignancies, specifically MM. After careful review of literature, since early 2018, we changed our clinical practice and routinely placed newly diagnosed MM (NDMM) patients receiving KRD at Memorial Sloan Kettering Cancer Center (MSKCC) on concomitant rivaroxaban 10 mg once daily, regardless of VTE risk stratification. In the following abstract, we present VTE rates and safety data for newly diagnosed MM patients receiving RVD with ASA vs. KRD with ASA vs. KRD with rivaroxaban prophylaxis.
Methods
This was an IRB-approved, single-center, retrospective chart review study. All untreated patients with newly diagnosed MM, receiving at least one cycle of RVD or KRD between January 2015 and October 2018 were included. The period of observation included the time between the first day of therapy until 90 days after completion of induction therapy. Patients were identified by querying the pharmacy database for carfilzomib or bortezomib administration and outpatient medication review of thromboprophylaxis with rivaroxaban or ASA. VTE diagnoses were confirmed by ICD-10 codes and appropriate imaging studies (computed tomography and ultrasound). Descriptive statistics were performed.
Results
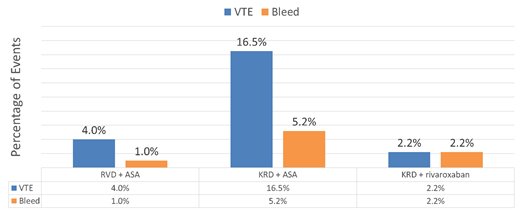
During the observation period, 241 patients were identified to have received RVD or KRD in the frontline (99 RVD with ASA; 97 KRD with ASA; 45 KRD with rivaroxaban). Baseline characteristics were well distributed among the three arms, with a median age of 60 (30-94) in the RVD ASA arm, 62 (33-77) in the KRD ASA arm, and 60 (24-79) in the KRD rivaroxaban arm. Patients had International Staging System (ISS) stage 3 disease in 13% (N=13), 9.3% (N=9), and 11% (N=5) of the RVD ASA, KRD ASA, and KRD rivaroxaban arms, respectively. Median weekly doses of dexamethasone were higher in both KRD arms, 40 mg (20-40) vs. 20 mg (10-40) in the RVD ASA arm. The average initial doses of lenalidomide were 22 mg in the RVD ASA arm compared to 25 mg in both the KRD ASA and KRD rivaroxaban arms. After querying the pharmacy database, no patients were identified to have a history or concomitant use of erythropoietin stimulating agent (ESA) use. Treatment-related VTE's occurred in 4 patients (4.0%) in the RVD ASA arm, 16 patients (16.5%) in the KRD ASA arm, and in 1 patient (2.2%) in the KRD rivaroxaban arm. Average time to VTE was 6.15 months (Range 5.42, 9.73) after treatment initiation in the RVD ASA group, while it was 2.61 months (Range 0.43, 5.06) in the KRD ASA group and 1.35 months in the KRD rivaroxaban group. Minor, grade 1 bleeding events per the Common Terminology Criteria for Adverse Events (CTCAE) were identified in 1 (1.1%) patient in the RVD ASA arm, 5 (5.2%) patients in the KRD ASA arm, and 1 (2.2%) patient in the KRD rivaroxaban arm.
Conclusion
More efficacious MM combination therapies have been found to increase the risk of VTE when using ASA prophylaxis, indicating better thromboprophylaxis is needed. We found patients receiving ASA prophylaxis with KRD were more likely to experience a VTE and these events occurred earlier compared to patients receiving ASA prophylaxis with RVD. Importantly, the rate of VTE was reduced to the same level as ASA prophylaxis with RVD when low-dose rivaroxaban 10 mg daily was used with KRD, and without necessarily increasing bleeding risk. Our retrospective data support the development of prospective clinical trials further investigating DOAC use in thromboprophylaxis for NDMM patients receiving carfilzomib-based treatments.
Hassoun:Novartis: Consultancy; Janssen: Research Funding; Celgene: Research Funding. Lesokhin:BMS: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria; Janssen: Research Funding; GenMab: Consultancy, Honoraria; Serametrix Inc.: Patents & Royalties; Genentech: Research Funding; Juno: Consultancy, Honoraria. Mailankody:Juno: Research Funding; Celgene: Research Funding; Janssen: Research Funding; Takeda Oncology: Research Funding; CME activity by Physician Education Resource: Honoraria. Smith:Celgene: Consultancy, Patents & Royalties, Research Funding; Fate Therapeutics and Precision Biosciences: Consultancy. Landgren:Theradex: Other: IDMC; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Abbvie: Membership on an entity's Board of Directors or advisory committees; Karyopharm: Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Merck: Other: IDMC; Sanofi: Membership on an entity's Board of Directors or advisory committees; Adaptive: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding.
Off-label use of rivaroxaban for outpatient prophylaxis of venous thromboembolism (VTE) will be explicitly disclosed to the audience.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal