

Background: Circulating cell-free DNA (ccfDNA) is highly fragmented DNA in plasma that is released by normal or tumor cells when they undergo apoptosis or necrosis. ccfDNA allows for non-invasive sampling of somatic genomic alterations and is informative in various solid tumors, including as a marker of measurable residual disease (MRD). We sought to assess the utility of baseline assessment and tracking of leukemia-associated mutations through peripheral blood sampling of ccfDNA in patients (pts) with acute leukemias.
Methods: Plasma ccfDNA was isolated and analyzed using a next-generation sequencing (NGS) assay of 275 genes. This NGS analysis is based on Single Primer Extension library preparation with unique molecular identifier (Qiagen, Germantown, MD); a sequence coverage ≥ 100X (after removing duplicates) was required. Amplicon-based NGS was also performed on DNA extracted from the bone marrow (BM) in a CLIA-certified molecular diagnostics laboratory. This BM panel detects mutations in the coding sequence of 28 leukemia-associated genes, with an analytic sensitivity of 5-10%. The ccfDNA panel included all 28 genes evaluated on the BM NGS panel (ABL1, ASXL1, BRAF, DNMT3A, EGFR, EZH2, FLT3, GATA1, GATA2, HRAS, IDH1, IDH2, IKZF1, JAK2, KIT, KRAS, MDM2, MLL, MPL, MYD88, NOTCH1, NPM1, NRAS, PTPN11, RUNX1, TET2, TP53, WT1). Established bioinformatics pipelines were used to identify somatic variants.
Results: Twenty-four pts (AML, n=22; ALL, n=2) underwent paired ccfDNA and BM sequencing at diagnosis prior to receiving frontline intensive chemotherapy. For baseline samples, ccfDNA was collected a median of 6 days after BM collection (range, 0-27 days) and a median of 0.5 days after start of induction chemotherapy (range, -7 to 7 days). Eleven pts (46%) also had ccfDNA collected at ≥1 time point during remission.
Among the 28 genes of interest, the median number of mutations per pt detected in BM and in ccfDNA was 1 (range, 0-4) for both assays (P=0.39). A total of 40 mutations were detected: 18 mutations (45%) were detected by both methods, 7 (18%) were detected only in ccfDNA, and 15 (38%) were detected only in BM. Time from start of chemotherapy until ccfDNA collection did not appear to impact the concordance of ccfDNA and BM mutation analysis (P=0.87).
Among mutations detected by ccfDNA in baseline samples, the median variant allelic frequency (VAF) was 33.7% (range, 2.7-90.8%). Among the 18 overlapping mutations, the concordance of VAF assessment by both methods was high (R2 = 0.849). Mutations detected by only one of the two methods were generally of lower VAF than those detected by both methods, suggesting that either method may miss small subclonal populations. The median VAF of mutations (as measured in ccfDNA) that were detected by both methods was higher than those detected only in ccfDNA (39.8% vs 25.2%, respectively; P=0.04); similarly, the median VAF of mutations (as measured in BM) that were detected by both methods was higher than those detected only in BM (40.2% vs 6.6%; P=0.001).
Among the 7 mutations detected only by ccfDNA, ASXL1 was detected in 2 pts, WT1 in 1 pt, IDH1 in 1 pt, and BRAF and two EGFR mutations in 1 pt. Among the 5 pts in whom mutations were detected in ccfDNA but not BM, 2 eventually relapsed. In both pts, the discordant mutation (IDH1 and ASXL1) was detected in the relapse BM, suggesting that these were true mutations that were missed by NGS of the baseline BM.
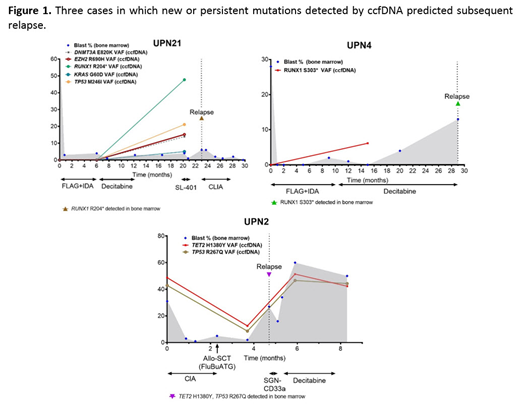
ccfDNA detected leukemia-associated mutations during remission that appeared to herald overt relapse (Figure 1). Two pts with t(8;21) AML developed new RUNX1 mutations detected by ccfDNA while in remission and subsequently relapsed 3 months and 14 months later. In both of these pts, the new RUNX1 mutation was confirmed in the BM at the time of morphological relapse. Another pt with AML had persistent TP53 and TET2 mutations detected by ccfDNA 1 month after allogeneic stem cell transplant and subsequently relapsed 1 month later.
Conclusions: This study demonstrates that sequencing of ccfDNA can identify prognostic or targetable mutations not detected by BM NGS. However, true mutations were missed by both ccfDNA and BM analysis, suggesting that these methodologies may be complementary in the assessment and monitoring of pts with leukemia. The use of ccfDNA as a non-invasive method to detect mutations and track MRD in AML and other leukemias should be evaluated in larger, prospective cohorts.
Short:Takeda Oncology: Consultancy, Research Funding; AstraZeneca: Consultancy; Amgen: Honoraria. Jabbour:Amgen: Consultancy, Research Funding; BMS: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Cyclacel LTD: Research Funding; AbbVie: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding; Takeda: Consultancy, Research Funding. Garcia-Manero:Amphivena: Consultancy, Research Funding; Helsinn: Research Funding; Novartis: Research Funding; AbbVie: Research Funding; Celgene: Consultancy, Research Funding; Astex: Consultancy, Research Funding; Onconova: Research Funding; H3 Biomedicine: Research Funding; Merck: Research Funding. Kantarjian:BMS: Research Funding; Amgen: Honoraria, Research Funding; Agios: Honoraria, Research Funding; Immunogen: Research Funding; Takeda: Honoraria; Novartis: Research Funding; Ariad: Research Funding; Astex: Research Funding; Pfizer: Honoraria, Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Daiichi-Sankyo: Research Funding; Jazz Pharma: Research Funding; Cyclacel: Research Funding; AbbVie: Honoraria, Research Funding. Ravandi:Macrogenix: Consultancy, Research Funding; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Xencor: Consultancy, Research Funding; Menarini Ricerche: Research Funding; Cyclacel LTD: Research Funding; Selvita: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal