

Key Points
Oral-AZA significantly improved overall and RFS vs placebo independent of baseline MRD status.
Rate of MRD+ to MRD− conversion was higher with oral-AZA; one-fourth of MRD responders achieved MRD negativity >6 months after starting oral-AZA.

Abstract
Measurable residual disease (MRD) in patients with acute myeloid leukemia (AML) in remission after intensive chemotherapy is predictive of early relapse and poor survival. Postremission maintenance therapy that prolongs MRD negativity or converts MRD+ patients to MRD− status may delay or prevent relapse and improve overall survival (OS). In the phase 3 QUAZAR AML-001 trial, oral azacitidine (oral-AZA; formerly CC-486), a hypomethylating agent, significantly prolonged OS and relapse-free survival (RFS) compared with placebo in patients aged ≥55 years with AML in first remission after intensive chemotherapy who were not candidates for hematopoietic stem cell transplantation. In this trial, MRD (≥0.1% leukemic cells in bone marrow) was assessed by multiparameter flow cytometry in serial samples collected at baseline and on day 1 of every 3 cycles. As expected, baseline MRD status was significantly associated with both OS and RFS. Multivariate analyses showed oral-AZA significantly improved OS and RFS vs placebo independent of baseline MRD status. Oral-AZA treatment also extended the duration of MRD negativity by 6 months vs placebo and resulted in a higher rate of conversion from MRD+ at baseline to MRD− during treatment: 37% vs 19%, respectively. In the oral-AZA arm, 24% of MRD responders achieved MRD negativity >6 months after treatment initiation. Although presence or absence of MRD was a strong prognostic indicator of OS and RFS, there were added survival benefits with oral-AZA maintenance therapy compared with placebo, independent of patients’ MRD status at baseline. Registered at clinicaltrials.gov as #NCT01757535.
Introduction
In newly diagnosed acute myeloid leukemia (AML), high remission rates are achieved with intensive chemotherapy (IC), but remissions are often transient.1 A variety of therapies, including hypomethylating agents, have been investigated in clinical trials for use as maintenance therapy in patients with AML in remission. Although some therapies in the maintenance setting have been shown to prolong disease-free or relapse-free survival (RFS) after IC, until recently, none has shown a significant impact on overall survival (OS) in a large, randomized study.2-11 Oral azacitidine (oral-AZA; formerly CC-486) is a hypomethylating agent that allows for extended dosing schedules to prolong drug exposure over each treatment cycle.12,13 Oral-AZA has a distinct pharmacokinetic and pharmacodynamic profile from that of injectable azacitidine, and the 2 formulations are not bioequivalent nor interchangeable.12,14 In the randomized, phase 3 QUAZAR AML-001 trial (clinicaltrials.gov #NCT01757535), treatment with oral-AZA significantly prolonged median OS by 9.9 months vs placebo (24.7 vs 14.8 months, respectively) and median RFS by 5.3 months (10.2 vs 4.8 months) in patients aged ≥55 years with AML in first remission after induction chemotherapy, with or without subsequent consolidation, who were not considered candidates for hematopoietic cell transplant (HCT).15,16 Oral-AZA was generally well tolerated and did not diminish the favorable health-related quality of life for these patients, who at study entry reported levels of fatigue generally comparable to those of a healthy population.16,17 Based on these results, oral-AZA was recently approved in the United States, Canada, and the European Union for treatment of adult patients with AML in first remission following IC who are not able to complete intensive curative therapy (eg, HCT).18
The presence of measurable residual disease (MRD) in patients with AML in remission after IC has consistently been shown to be predictive of relapse19-22 and is an adverse prognostic indicator that may help guide treatment decisions.21,22 Accordingly, the ability to prolong MRD negativity and to convert patients who are MRD+after IC to MRD− status may be important features of an effective AML maintenance strategy, but until recently, prospective data were lacking.23-25 For patients who are MRD−, maintenance therapy could theoretically suppress the emergence of resistant clonal populations that may ultimately lead to disease relapse. For MRD+ patients, an ideal therapy would promote conversion to MRD negativity, potentially delaying overt relapse and improving OS.21,22,26,27
MRD can be assessed using multiparameter flow cytometry (MFC), real-time quantitative polymerase chain reaction (PCR), digital droplet PCR, or next-generation sequencing technologies. Using MFC, MRD is determined by (1) tracking leukemia-associated aberrant immunophenotypes defined at diagnosis, (2) using a different-from-normal (DfN) approach that assesses immunophenotypic shifts at subsequent timepoints during remission, or (3) using a combined leukemia-associated aberrant immunophenotypes–based DfN approach when diagnostic samples are available. The combined approach is applicable for the vast majority of patient samples and is currently recommended by the European LeukemiaNet MRD Working Party, with a prognostic significance threshold of ≥0.1% for MRD positivity.22
Given the prognostic impact of MRD in AML,19-22 we assessed MRD (an exploratory study endpoint) by MFC in samples collected at screening and serially during treatment in the QUAZAR AML-001 trial. In univariate analysis, OS and RFS benefits were observed with oral-AZA vs placebo within both subgroups defined by the presence of MRD at screening (MRD+ or MRD−). Here, we further assess survival endpoints based on MRD status at screening, conversion from MRD+ to MRD− during treatment, and the durability of MRD negativity while on treatment.
Methods
Trial design and patient eligibility
Trial design and key inclusion and exclusion criteria have been reported in detail.16 Briefly, eligible patients were aged ≥55 years, with intermediate- or poor-risk cytogenetics at diagnosis (according to the National Comprehensive Cancer Network 2011 AML Guidelines28), had achieved first complete remission (CR) or CR with incomplete hematologic recovery (CRi) (International Working Group 2003 AML criteria29) after intensive chemotherapy (induction plus or minus consolidation), and were not considered candidates for HCT by their treating physician before study screening. The use and type of consolidation therapy were determined by the treating physician and occurred prior to study screening, and patients were eligible for enrollment regardless of whether or not they received consolidation.
Within 4 months (plus or minus 7 days) of achieving CR/CRi, patients were randomized 1:1 to receive oral-AZA 300 mg or placebo once daily on days 1 to 14 of repeated 28-day treatment cycles. Randomization was stratified by age, prior history of myelodysplastic syndromes or chronic myelomonocytic leukemia, cytogenetic risk at diagnosis, and receipt of consolidation chemotherapy. Baseline MRD status was established using the initial bone marrow aspirate taken at the time of screening (after completion of induction plus or minus consolidation and ≤28 days before randomization). The data cutoff date was 15 July 2019.
MRD assessments
The MRD− evaluable cohort consisted of all patients who had bone marrow samples available for MFC evaluation at baseline and at ≥1 postbaseline visit. MFC assessments were performed centrally by Münchner Leukämielabor, GmbH (Munich, Germany) as previously described.30-32 The flow cytometry MRD assay was run in real time on fresh patient bone marrow aspirate samples collected at baseline (screening) on day 1 (plus or minus 7 days) of every 3 cycles, up to cycle 24, and every 6 cycles thereafter, and as clinically indicated.15 Samples from the time of AML diagnosis or from the time of achievement of CR/CRi were not available for assessment. The MFC MRD assay was run using a set of 22 cell-surface markers (supplemental Table 1), and MRD was quantified using a DfN approach with an MRD+ cutoff of ≥0.1%, consistent with the 2017 European LeukemiaNet guidelines.22 The assay was performed in 7 separate tubes, each with 5 unique marker combinations, along with standard forward scatter and side scatter measurements.
Statistical analysis
The primary and key secondary endpoints of the QUAZAR AML-001 trial were OS and RFS, respectively. OS was defined as the time from randomization to death from any cause, and RFS was defined as the interval from the date of randomization to the date of AML relapse (ie, ≥5% blasts in bone marrow by morphological analysis) or death from any cause. MRD was not used to define relapse. Patients who were still alive without documented relapse, or who were lost to follow-up without documented relapse, were censored at the date of their last response assessment. Survival outcomes were assessed within subgroups of patients defined by MRD status at study entry (MRD+ or MRD−), and for patients who were MRD+ at baseline and achieved an MRD response on study (defined below). OS, RFS, and duration of MRD negativity were estimated using Kaplan-Meier methods. All MRD analyses were exploratory endpoints; relative hazard ratios (HRs) for OS and RFS comparisons between treatment arms within MRD-based subgroups are provided, but analyses were not powered to detect statistical significance.
Multivariate analyses were performed to evaluate the effect of baseline MRD status (MRD+ vs MRD−) on OS and RFS independent of randomized treatment arm (oral-AZA vs placebo) and of treatment arm independent of MRD status. HRs and 95% confidence intervals (CIs) for multivariate analyses were calculated using a Cox proportional hazards regression model, and P values were determined by Wald tests.
MRD response and duration of MRD negativity
Conversion of MRD status (ie, MRD− to MRD+ or MRD+ to MRD−) was noted if there were 2 consecutive MRD assessments at the new status. For example, for patients who were MRD+ at baseline (≥0.1% MRD by MFC), MRD response was defined as achievement of MRD negativity for ≥2 consecutive assessments during the randomized treatment phase. Duration of MRD negativity was calculated as the time between randomization (for patients MRD− at baseline) or the first of ≥2 consecutive on-treatment MRD− tests (for MRD responders) until the first of 2 consecutive MRD+ assessments or treatment discontinuation. For patients with discontinuous periods of confirmed MRD negativity, MRD− duration was the sum of all MRD− periods, excluding the duration of any intervening MRD+ intervals. Missing longitudinal data did not change MRD status unless the time interval between the 2 MRD measurements exceeded 200 days; in this case, an MRD+ value was assumed for the entire gap as a conservative approach. Examples of how MRD duration and conversion were calculated in different scenarios are shown in supplemental Figure 1.
Results
Patient disposition and baseline characteristics
The MRD-evaluable cohort comprised 463/472 (98.1%) randomized patients (oral-AZA, n = 236; placebo, n = 227) with bone marrow samples available for MFC evaluation at baseline and at ≥1 postbaseline visit (supplemental Figure 2). At baseline, 44% of evaluable patients (n = 103) in the oral-AZA arm and 51% (n = 116) in the placebo arm were MRD+. The majority of MRD+ patients (132/219 [60%]) had < 0.5% leukemic cells at baseline (Table 1). Median bone marrow blast percent by cytomorphology at baseline for MRD+ patients was 2.5% (range, 0.0 to 5.0) in the oral-AZA arm and 2.0% (0.0 to 6.5) in the placebo arm (patients may have had multiple visits between screening and randomization, but all patients met relevant eligibility criteria at their screening visit) and was 1.5% (0.0 to 4.5) and 2.0% (0.0 to 4.5), respectively, in the MRD− subgroup. Overall, baseline characteristics were generally similar between MRD+ and MRD− patients: median ages were 69 (range 55 to 84) and 68 (55 to 86) years, respectively; 84% and 88% of patients had intermediate-risk cytogenetics at diagnosis, 52% and 46% had an Eastern Cooperative Oncology Group performance status score of 0, 83% and 79% were in CR (rather than CRi) post-IC, and 79% and 82% received consolidation after induction (Table 2). There was no significant association between the number of consolidation courses received before study entry (0, 1, or 2 to 3) and the likelihood of being MRD+ or MRD− at baseline (χ-squared P = .36). There were few notable differences in baseline characteristics between treatment arms within each MRD cohort; however, within the subgroup of patients who were MRD− at baseline, a greater proportion of patients in the placebo arm than in the oral-AZA arm had achieved CR (as opposed to CRi) after induction (87% vs 72%, respectively; P = .004).
MRD status at randomization and degree of MRD positivity as a percentage of leukemic cells in bone marrow aspirates
| Group | N | MRD− (<0.1%) | MRD+ (≥0.1%) | Degree of MRD positivity | ||
|---|---|---|---|---|---|---|
| 0.1-0.5% | ≥0.5-1.0% | >1.0% | ||||
| n (%) | ||||||
| All patients | 463 | 244 (53) | 219 (47) | 132 (29) | 36 (8) | 51 (11) |
| Oral azacitidine | 236 | 133 (56) | 103 (44) | 63 (27) | 16 (7) | 24 (10) |
| Placebo | 227 | 111 (49) | 116 (51) | 69 (30) | 20 (9) | 27 (12) |
| Group | N | MRD− (<0.1%) | MRD+ (≥0.1%) | Degree of MRD positivity | ||
|---|---|---|---|---|---|---|
| 0.1-0.5% | ≥0.5-1.0% | >1.0% | ||||
| n (%) | ||||||
| All patients | 463 | 244 (53) | 219 (47) | 132 (29) | 36 (8) | 51 (11) |
| Oral azacitidine | 236 | 133 (56) | 103 (44) | 63 (27) | 16 (7) | 24 (10) |
| Placebo | 227 | 111 (49) | 116 (51) | 69 (30) | 20 (9) | 27 (12) |
MRD, measurable residual disease.
Demographic and disease characteristics in the MRD-evaluable cohort, stratified by MRD status at baseline and by randomized treatment arm
| Baseline MRD+ | Baseline MRD− | |||||
|---|---|---|---|---|---|---|
| Characteristic | Oral azacitidine (n = 103) | Placebo (n = 116) | Total (n = 219) | Oral azacitidine (n = 133) | Placebo (n = 111) | Total (n = 244) |
| Age, years, median (range) | 68 (55-84) | 69 (56-82) | 69 (55-84) | 68 (56-86) | 68 (55-79) | 68 (55-86) |
| Sex, n (%) | ||||||
| Male | 50 (49) | 60 (52) | 110 (50) | 67 (50) | 64 (58) | 131 (54) |
| Female | 53 (51) | 56 (48) | 109 (50) | 66 (50) | 47 (42) | 113 (46) |
| WHO AML classification, n (%) | ||||||
| Recurrent genetic abnormalities | 17 (17) | 19 (16) | 36 (16) | 22 (17) | 24 (22) | 46 (19) |
| Myelodysplasia-related changes | 19 (18) | 26 (22) | 45 (21) | 29 (22) | 14 (13) | 43 (18) |
| Therapy-related | 2 (2) | 0 | 2 (0.9) | 0 | 0 | 0 |
| Not otherwise specified | 65 (63) | 71 (61) | 136 (62) | 82 (62) | 72 (65) | 154 (63) |
| Missing | 0 | 0 | 0 | 0 | 1 (0.9) | 1 (0.4) |
| Type of AML, n (%) | ||||||
| De novo | 90 (87) | 106 (91) | 196 (89) | 122 (92) | 103 (93) | 225 (92) |
| Secondary | 13 (13) | 10 (9) | 23 (11) | 11 (8) | 8 (7) | 19 (8) |
| Prior history of MDS/CMML, n (%) | 10 (10) | 9 (8) | 19 (9) | 11 (8) | 8 (7) | 19 (8) |
| Cytogenetic risk at diagnosis, n (%) | ||||||
| Intermediate | 87 (84) | 97 (84) | 184 (84) | 114 (86) | 100 (90) | 214 (88) |
| Poor | 16 (16) | 19 (16) | 35 (16) | 19 (14) | 11 (10) | 30 (12) |
| Response following induction, n (%) | ||||||
| CR | 89 (86) | 93 (80) | 182 (83) | 96 (72) | 97 (87) | 193 (79) |
| CRi | 14 (14) | 23 (20) | 37 (17) | 37 (28) | 14 (13) | 51 (21) |
| Received consolidation therapy, n (%) | ||||||
| Yes | 82 (80) | 90 (78) | 172 (79) | 103 (77) | 96 (86) | 199 (82) |
| 1 cycle | 51 (50) | 52 (45) | 103 (47) | 58 (44) | 49 (44) | 107 (44) |
| 2 cycles | 28 (27) | 32 (28) | 60 (27) | 42 (32) | 40 (36) | 82 (34) |
| 3 cycles | 3 (3) | 6 (5) | 9 (4) | 3 (2.3) | 7 (6) | 10 (4) |
| No | 21 (20) | 26 (22) | 47 (22) | 30 (23) | 15 (14) | 45 (18) |
| Total number of chemotherapy cycles received (induction + consolidation), median (range) | 2 (1-7) | 2 (1-6) | 2 (1-7) | 2 (1-6) | 2 (1-5) | 2 (1-6) |
| Response at randomization, n (%) | ||||||
| CR | 85 (83) | 87 (75) | 172 (79) | 97 (73) | 85 (77) | 182 (75) |
| CRi | 16 (16) | 23 (20) | 39 (18) | 33 (25) | 20 (18) | 53 (22) |
| No longer in CR/CRi | 2 (2) | 5 (4) | 7 (3) | 3 (2) | 6 (5) | 9 (4) |
| Missing | 0 | 1 (0.9) | 1 (0.5) | 0 | 0 | 0 |
| Time from diagnosis to randomization, months, median (range) | 4.2 (1.7-9.2) | 4.1 (1.5-7.6) | 4.1 (1.5-9.2) | 4.2 (1.5-9.1) | 4.3 (1.4-10.9) | 4.3 (1.4-10.9) |
| Time from induction to randomization, months, median (range) | 4.0 (1.5-7.8) | 3.9 (1.5-15.1) | 4.0 (1.5-15.1) | 3.9 (1.4-8.8) | 4.0 (1.3-10.2) | 4.0 (1.3-10.2) |
| Time from achievement of CR/CRi to randomization, days, median (range)* | 81 (7-130) | 80 (7-134) | 81 (7-134) | 85 (8-154) | 87 (11-263) | 86 (8-263) |
| ECOG performance status score, n (%) | ||||||
| 0 | 56 (54) | 57 (49) | 113 (52) | 59 (44) | 52 (47) | 111 (46) |
| 1 | 40 (39) | 49 (42) | 89 (41) | 61 (46) | 52 (47) | 113 (46) |
| 2-3 | 7 (7) | 10 (9) | 17 (8) | 13 (10) | 7 (6) | 20 (8) |
| Reason ineligible for HSCT, n (%)† | ||||||
| Age | 68 (66) | 78 (67) | 146 (67) | 85 (64) | 69 (62) | 154 (63) |
| Comorbidities | 28 (27) | 24 (21) | 52 (24) | 24 (18) | 23 (21) | 47 (19) |
| Performance status | 6 (6) | 4 (3) | 10 (5) | 7 (5) | 4 (4) | 11 (5) |
| No available donor | 12 (12) | 19 (16) | 31 (14) | 25 (19) | 16 (14) | 41 (17) |
| Patient decision | 4 (4) | 13 (11) | 17 (8) | 15 (11) | 19 (17) | 34 (14) |
| Unfavorable cytogenetics | 2 (2) | 2 (2) | 4 (2) | 4 (3) | 8 (7) | 12 (5) |
| Other | 13 (13) | 8 (7) | 21 (10) | 14 (11) | 11 (10) | 25 (10) |
| Bone marrow blasts, %, median (range)‡ | 2.5 (0.0-5.0) | 2.0 (0.0-6.5) | 2.5 (0.0-6.5) | 1.5 (0.0-4.5) | 2.0 (0.0-4.5) | 2.0 (0.0-4.5) |
| Hemoglobin, g/L, median (range) | 113 (86-159) | 109 (77-149) | 111 (77-159) | 115 (75-149) | 109 (81-140) | 111 (75-149) |
| Platelets, 109/L, median (range)‡ | 163 (29-735) | 184 (23-636) | 174 (23-735) | 145 (22-801) | 173 (21-626) | 160 (21-801) |
| Platelet count <50 ×109/L, n (%) | 4 (4) | 9 (8) | 13 (6) | 8 (6) | 7 (6) | 15 (6) |
| ANC, 109/L, median (range)‡ | 3.4 (0.6-15.6) | 2.6 (0.5-9.6) | 3.1 (0.5-15.6) | 2.6 (0.3-15.9) | 3.0 (0.6-9.1) | 2.8 (0.3-15.9) |
| ANC <1.0 ×109/L, n (%) | 4 (4) | 8 (7) | 12 (6) | 3 (2) | 10 (9) | 13 (5) |
| WBC, 109/L, median (range) | 5.3 (1.5-18.0) | 4.5 (1.7-12.6) | 4.9 (1.5-18.0) | 4.6 (0.8-18.7) | 4.5 (1.3-12.2) | 4.5 (0.8-18.7) |
| Baseline MRD+ | Baseline MRD− | |||||
|---|---|---|---|---|---|---|
| Characteristic | Oral azacitidine (n = 103) | Placebo (n = 116) | Total (n = 219) | Oral azacitidine (n = 133) | Placebo (n = 111) | Total (n = 244) |
| Age, years, median (range) | 68 (55-84) | 69 (56-82) | 69 (55-84) | 68 (56-86) | 68 (55-79) | 68 (55-86) |
| Sex, n (%) | ||||||
| Male | 50 (49) | 60 (52) | 110 (50) | 67 (50) | 64 (58) | 131 (54) |
| Female | 53 (51) | 56 (48) | 109 (50) | 66 (50) | 47 (42) | 113 (46) |
| WHO AML classification, n (%) | ||||||
| Recurrent genetic abnormalities | 17 (17) | 19 (16) | 36 (16) | 22 (17) | 24 (22) | 46 (19) |
| Myelodysplasia-related changes | 19 (18) | 26 (22) | 45 (21) | 29 (22) | 14 (13) | 43 (18) |
| Therapy-related | 2 (2) | 0 | 2 (0.9) | 0 | 0 | 0 |
| Not otherwise specified | 65 (63) | 71 (61) | 136 (62) | 82 (62) | 72 (65) | 154 (63) |
| Missing | 0 | 0 | 0 | 0 | 1 (0.9) | 1 (0.4) |
| Type of AML, n (%) | ||||||
| De novo | 90 (87) | 106 (91) | 196 (89) | 122 (92) | 103 (93) | 225 (92) |
| Secondary | 13 (13) | 10 (9) | 23 (11) | 11 (8) | 8 (7) | 19 (8) |
| Prior history of MDS/CMML, n (%) | 10 (10) | 9 (8) | 19 (9) | 11 (8) | 8 (7) | 19 (8) |
| Cytogenetic risk at diagnosis, n (%) | ||||||
| Intermediate | 87 (84) | 97 (84) | 184 (84) | 114 (86) | 100 (90) | 214 (88) |
| Poor | 16 (16) | 19 (16) | 35 (16) | 19 (14) | 11 (10) | 30 (12) |
| Response following induction, n (%) | ||||||
| CR | 89 (86) | 93 (80) | 182 (83) | 96 (72) | 97 (87) | 193 (79) |
| CRi | 14 (14) | 23 (20) | 37 (17) | 37 (28) | 14 (13) | 51 (21) |
| Received consolidation therapy, n (%) | ||||||
| Yes | 82 (80) | 90 (78) | 172 (79) | 103 (77) | 96 (86) | 199 (82) |
| 1 cycle | 51 (50) | 52 (45) | 103 (47) | 58 (44) | 49 (44) | 107 (44) |
| 2 cycles | 28 (27) | 32 (28) | 60 (27) | 42 (32) | 40 (36) | 82 (34) |
| 3 cycles | 3 (3) | 6 (5) | 9 (4) | 3 (2.3) | 7 (6) | 10 (4) |
| No | 21 (20) | 26 (22) | 47 (22) | 30 (23) | 15 (14) | 45 (18) |
| Total number of chemotherapy cycles received (induction + consolidation), median (range) | 2 (1-7) | 2 (1-6) | 2 (1-7) | 2 (1-6) | 2 (1-5) | 2 (1-6) |
| Response at randomization, n (%) | ||||||
| CR | 85 (83) | 87 (75) | 172 (79) | 97 (73) | 85 (77) | 182 (75) |
| CRi | 16 (16) | 23 (20) | 39 (18) | 33 (25) | 20 (18) | 53 (22) |
| No longer in CR/CRi | 2 (2) | 5 (4) | 7 (3) | 3 (2) | 6 (5) | 9 (4) |
| Missing | 0 | 1 (0.9) | 1 (0.5) | 0 | 0 | 0 |
| Time from diagnosis to randomization, months, median (range) | 4.2 (1.7-9.2) | 4.1 (1.5-7.6) | 4.1 (1.5-9.2) | 4.2 (1.5-9.1) | 4.3 (1.4-10.9) | 4.3 (1.4-10.9) |
| Time from induction to randomization, months, median (range) | 4.0 (1.5-7.8) | 3.9 (1.5-15.1) | 4.0 (1.5-15.1) | 3.9 (1.4-8.8) | 4.0 (1.3-10.2) | 4.0 (1.3-10.2) |
| Time from achievement of CR/CRi to randomization, days, median (range)* | 81 (7-130) | 80 (7-134) | 81 (7-134) | 85 (8-154) | 87 (11-263) | 86 (8-263) |
| ECOG performance status score, n (%) | ||||||
| 0 | 56 (54) | 57 (49) | 113 (52) | 59 (44) | 52 (47) | 111 (46) |
| 1 | 40 (39) | 49 (42) | 89 (41) | 61 (46) | 52 (47) | 113 (46) |
| 2-3 | 7 (7) | 10 (9) | 17 (8) | 13 (10) | 7 (6) | 20 (8) |
| Reason ineligible for HSCT, n (%)† | ||||||
| Age | 68 (66) | 78 (67) | 146 (67) | 85 (64) | 69 (62) | 154 (63) |
| Comorbidities | 28 (27) | 24 (21) | 52 (24) | 24 (18) | 23 (21) | 47 (19) |
| Performance status | 6 (6) | 4 (3) | 10 (5) | 7 (5) | 4 (4) | 11 (5) |
| No available donor | 12 (12) | 19 (16) | 31 (14) | 25 (19) | 16 (14) | 41 (17) |
| Patient decision | 4 (4) | 13 (11) | 17 (8) | 15 (11) | 19 (17) | 34 (14) |
| Unfavorable cytogenetics | 2 (2) | 2 (2) | 4 (2) | 4 (3) | 8 (7) | 12 (5) |
| Other | 13 (13) | 8 (7) | 21 (10) | 14 (11) | 11 (10) | 25 (10) |
| Bone marrow blasts, %, median (range)‡ | 2.5 (0.0-5.0) | 2.0 (0.0-6.5) | 2.5 (0.0-6.5) | 1.5 (0.0-4.5) | 2.0 (0.0-4.5) | 2.0 (0.0-4.5) |
| Hemoglobin, g/L, median (range) | 113 (86-159) | 109 (77-149) | 111 (77-159) | 115 (75-149) | 109 (81-140) | 111 (75-149) |
| Platelets, 109/L, median (range)‡ | 163 (29-735) | 184 (23-636) | 174 (23-735) | 145 (22-801) | 173 (21-626) | 160 (21-801) |
| Platelet count <50 ×109/L, n (%) | 4 (4) | 9 (8) | 13 (6) | 8 (6) | 7 (6) | 15 (6) |
| ANC, 109/L, median (range)‡ | 3.4 (0.6-15.6) | 2.6 (0.5-9.6) | 3.1 (0.5-15.6) | 2.6 (0.3-15.9) | 3.0 (0.6-9.1) | 2.8 (0.3-15.9) |
| ANC <1.0 ×109/L, n (%) | 4 (4) | 8 (7) | 12 (6) | 3 (2) | 10 (9) | 13 (5) |
| WBC, 109/L, median (range) | 5.3 (1.5-18.0) | 4.5 (1.7-12.6) | 4.9 (1.5-18.0) | 4.6 (0.8-18.7) | 4.5 (1.3-12.2) | 4.5 (0.8-18.7) |
ANC, absolute neutrophil count; CMML, chronic myelomonocytic leukemia; ECOG, Eastern Cooperative Oncology Group; HSCT, hematopoietic stem cell transplant; MDS, myelodysplastic syndromes; WBC, white blood cell count; WHO, World Health Organization.
4 patients were enrolled beyond the 4-month (plus or minus 7 days) inclusion window (protocol violations).
Patients may have been accounted for in multiple categories.
Patients may have had multiple visits between screening and randomization. All patients met relevant eligibility criteria at their screening visit.
Baseline MRD status was prognostic of survival
Within each treatment arm, median OS was substantially shorter in patients who were MRD+ at baseline than for those who were MRD− (Figure 1), confirming the adverse prognostic impact of the MFC-defined ≥0.1% MRD+ threshold; the HR for OS between the MRD+ and MRD− subgroups was 1.7 (95% CI, 1.3, 2.4) in the oral-AZA arm and 1.9 (1.5, 2.7) in the placebo arm. Similarly, RFS was reduced in patients who were MRD+ at baseline in both the oral-AZA (HR, 1.8 [95% CI, 1.4, 2.5] vs MRD−) and placebo (2.2 [1.7, 3.0]) arms. Multivariate analysis confirmed the significant independent association of MRD status at baseline (MRD+ vs MRD−) with OS (HR, 1.85 [95% CI, 1.49, 2.31]) and RFS (HR, 2.04 [1.65, 2.53]) when controlling for treatment arm (oral-AZA or placebo) (Table 3).
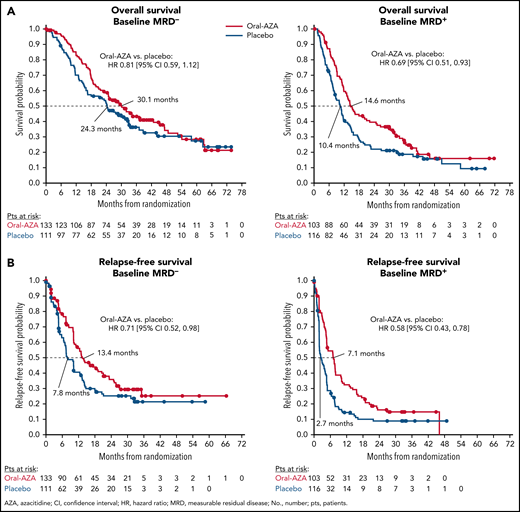
Kaplan-Meier estimated overall survival and relapse-free survival with oral azacitidine vs placebo by baseline measurable residual disease status (MRD+ or MRD−). (A) Overall survival; (B) Relapse-free survival.
Kaplan-Meier estimated overall survival and relapse-free survival with oral azacitidine vs placebo by baseline measurable residual disease status (MRD+ or MRD−). (A) Overall survival; (B) Relapse-free survival.
Multivariate analyses of OS and RFS, with baseline MRD status (MRD+ vs MRD−) and treatment arm (oral azacitidine vs placebo) included as covariates
| Parameter | HR [95% CI] | P value |
|---|---|---|
| Overall survival | ||
| Baseline MRD status | 1.85 [1.49, 2.31] | <.0001 |
| MRD+ vs MRD− | ||
| Treatment arm | 0.74 [0.59, 0.92] | .0067 |
| Oral-AZA vs placebo | ||
| Relapse-free survival | ||
| Baseline MRD status | 2.04 [1.65, 2.53] | <.0001 |
| MRD+ vs MRD− | ||
| Treatment arm | 0.63 [0.51, 0.78] | <.0001 |
| Oral-AZA vs placebo |
| Parameter | HR [95% CI] | P value |
|---|---|---|
| Overall survival | ||
| Baseline MRD status | 1.85 [1.49, 2.31] | <.0001 |
| MRD+ vs MRD− | ||
| Treatment arm | 0.74 [0.59, 0.92] | .0067 |
| Oral-AZA vs placebo | ||
| Relapse-free survival | ||
| Baseline MRD status | 2.04 [1.65, 2.53] | <.0001 |
| MRD+ vs MRD− | ||
| Treatment arm | 0.63 [0.51, 0.78] | <.0001 |
| Oral-AZA vs placebo |
AZA, azacitidine; CI, confidence interval; HR, hazard ratio; MRD, measurable residual disease; OS, overall survival; RFS, relapse-free survival.
Oral-AZA improved survival regardless of baseline MRD status
Treatment with oral-AZA was associated with improved OS from time of randomization compared with placebo regardless of post-IC MRD status: median OS for baseline MRD+ patients was 14.6 months with oral-AZA vs 10.4 months with placebo (HR, 0.69 [95% CI, 0.51, 0.93]) and was 30.1 vs 24.3 months, respectively, in patients who were MRD− at baseline (HR, 0.81 [0.59, 1.12]) (Figure 1A). Median RFS was also extended with oral-AZA vs placebo in both MRD subgroups: 7.1 vs 2.7 months, respectively, in baseline MRD+ patients (HR, 0.58 [95% CI, 0.43, 0.78]), and 13.4 vs 7.8 months in MRD− patients (0.71 [0.52, 0.98]) (Figure 1B). Multivariate analysis confirmed the significant independent benefit of treatment with oral-AZA vs placebo on both OS (HR, 0.74 [95% CI, 0.59, 0.92]) and RFS (0.63 [0.51, 0.78]) when controlling for baseline MRD status (Table 3).
Treatment with oral-AZA resulted in increased MRD responses
For baseline MRD+ patients, the conversion rate to MRD− status on study (ie, MRD response) was nearly twofold higher with oral-AZA (37%) than with placebo (19%) (odds ratio, 2.50 [95% CI, 1.35, 4.61]) (Table 4). The median time from randomization to first observed MRD− assessment for MRD responders was 61 days with oral-AZA and 59.5 days with placebo, which approximately corresponds to the 56-day interval between baseline and the first protocol-specified marrow assessment on day 1 of cycle 3. However, some patients treated with oral-AZA achieved an MRD response even after prolonged MRD positivity: 9/38 (24%) responders in the oral-AZA arm became MRD− >6 months after randomization (ranging up to 13.1 months) compared with only 1 patient (5%; at 8.1 months) in the placebo arm (Table 4; Figure 2).
Achievement of MRD response (MRD− at ≥2 consecutive assessments) among patients who were MRD+ at baseline
| Placebo | Oral-AZA | Placebo |
|---|---|---|
| MRD+ at baseline, N | 103 | 116 |
| MRD responders,* n (%) | 38/103 (37) | 22/116 (19) |
| OR [95% CI], Oral-AZA vs placebo | 2.50 [1.35, 4.61] | |
| Time to MRD response,*†n (%) | ||
| ≤3 mo | 22/38 (58) | 15/22 (68) |
| >3 to ≤6 mo | 7/38 (18) | 6/22 (27) |
| >6 mo | 9/38 (24) | 1/22 (5) |
| Placebo | Oral-AZA | Placebo |
|---|---|---|
| MRD+ at baseline, N | 103 | 116 |
| MRD responders,* n (%) | 38/103 (37) | 22/116 (19) |
| OR [95% CI], Oral-AZA vs placebo | 2.50 [1.35, 4.61] | |
| Time to MRD response,*†n (%) | ||
| ≤3 mo | 22/38 (58) | 15/22 (68) |
| >3 to ≤6 mo | 7/38 (18) | 6/22 (27) |
| >6 mo | 9/38 (24) | 1/22 (5) |
AZA, azacitidine; CI, confidence interval; mo, months; MRD, measurable residual disease; OR, odds ratio.
MRD response was defined as patients where were MRD+ at baseline and became MRD− on treatment.
Time from randomization.
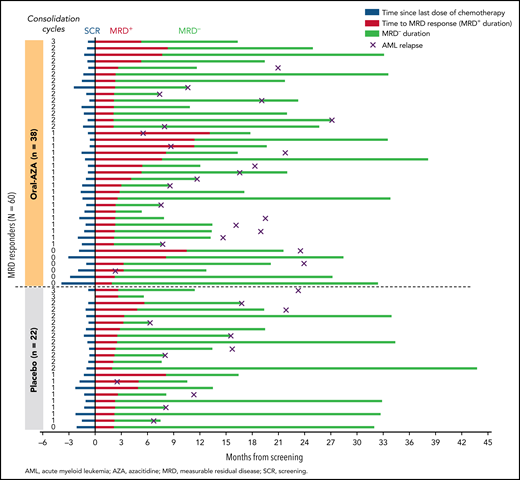
MRD responders: time between last dose of chemotherapy and screening, time to confirmed MRD negativity (ie, MRD+ duration), duration of MRD negativity, and time of confirmed relapse. Patients are sorted by randomized treatment arm and then in descending order by number of consolidation cycles. Some patients may have relapsed after discontinuing from the study (relapse date unknown).
MRD responders: time between last dose of chemotherapy and screening, time to confirmed MRD negativity (ie, MRD+ duration), duration of MRD negativity, and time of confirmed relapse. Patients are sorted by randomized treatment arm and then in descending order by number of consolidation cycles. Some patients may have relapsed after discontinuing from the study (relapse date unknown).
Achievement of MRD negativity on study was associated with longer survival: median OS for all MRD responders (n = 60) was 41.3 months compared with 9.0 months for those who remained MRD+ (n = 159) (HR, 0.21 [95% CI, 0.14, 0.32]). Similarly, median RFS was 20.4 months for MRD responders and 2.8 months for nonresponders (HR, 0.11 [95% CI, 0.07, 0.18]) (supplemental Table 2).
Duration of MRD negativity was prolonged by oral-AZA
Among all patients, the median total duration of MRD negativity at any time on study was prolonged by 6 months with oral-AZA vs placebo (11.0 vs 5.0 months, respectively) (Figure 3). Oral-AZA prolonged the duration of MRD negativity vs placebo for patients who were MRD− at baseline (median 26.4 vs 10.4 months, respectively), and for those who were MRD+ at baseline and achieved MRD− status on study (ie, MRD responders [median not reached vs 12.9 months]). The duration of MRD negativity was not clearly impacted by the number of consolidation cycles received (supplemental Figure 3). For the 178 patients who were MRD− at any time on study and had a subsequent documented AML relapse, the median time between the last MRD− assessment and date of AML relapse was 91 days (range, 1 to 428). Generally, longer aggregate duration of MRD− appeared to be associated with improved survival (supplemental Figure 1).
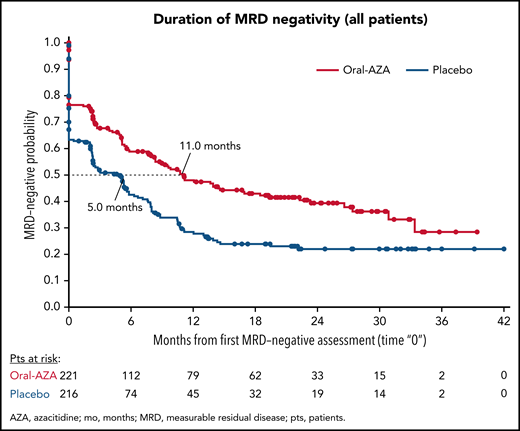
Kaplan-Meier estimated durations of MRD negativity during treatment with oral azacitidine and placebo, regardless of MRD status at baseline. Duration of “0” on the x-axis represents patients who never achieved protocol-defined MRD− status on study. Patients with missing or insufficient longitudinal data are not included in this analysis.
Kaplan-Meier estimated durations of MRD negativity during treatment with oral azacitidine and placebo, regardless of MRD status at baseline. Duration of “0” on the x-axis represents patients who never achieved protocol-defined MRD− status on study. Patients with missing or insufficient longitudinal data are not included in this analysis.
Characteristics of MRD responders
Among all baseline MRD+ patients, the median proportion of leukemic cells at baseline was 0.4%, and was the same for both MRD responders (n = 60) and those who remained MRD+ on study (n = 159). Median baseline MRD percent among MRD responders was also the same (0.4%) in both the oral-AZA and placebo arms (supplemental Figure 4). MRD responders received a median of 3 total cycles of chemotherapy (induction plus or minus consolidation) before study entry compared with 2 cycles for MRD+ nonresponders (supplemental Table 3), but the difference was not statistically significant (P = .40). As a group, MRD responders were more likely to have received consolidation therapy before study entry than those who remained MRD+ on study (88% vs 75%, respectively; P = .04); only 7 of 60 MRD responders (11.7%) did not receive consolidation after IC. Accordingly, the time from first CR/CRi during induction to study randomization was longer for MRD responders than nonresponders (median, 86.5 vs 77.0 days, respectively; P = .011). For patients who achieved an MRD response on study, there was no clear association between the number of consolidation cycles received or time since last dose of chemotherapy with time to achievement of MRD response (Figure 2).
In multivariate analyses of factors associated with MRD response within each treatment arm, there was a significant association between a higher number of prestudy consolidation cycles and attainment of an MRD response within the placebo arm (0 vs 1 vs 2 to 3; P = .0049), whereas MRD response in the oral-AZA arm was independent of the number of prior consolidation cycles (P = .45). Similarly, patients in the placebo arm were significantly less likely to attain an MRD response if they had poor-risk cytogenetics at diagnosis (P = .035), whereas cytogenetic risk did not influence attainment of an MRD response in the oral-AZA arm (P = .45) (supplemental Table 4). Conversely, presence of an NPM1 mutation at diagnosis was significantly predictive of achieving an MRD response in the oral-AZA arm (P = .0029) but not the placebo arm (P = .20). When including treatment arm as a covariate in the model, oral-AZA was significantly predictive of an MRD response compared with placebo (P = .0033) independent of all other variables in the model.
Discussion
The strong adverse prognostic impact of MRD positivity after IC has been established in retrospective studies and meta-analyses,21,25 but prospective, longitudinal MRD assessments in controlled trials of AML therapies have been scarce. The QUAZAR AML-001 trial is the largest randomized clinical trial of a novel agent to include prospective, long-term, central assessment of MRD in older patients with AML in remission. Nearly one-half of all patients enrolled in QUAZAR AML-001 were MRD+ at study entry by MFC assessment, generally similar to rates previously reported after AML treatment with IC.4,26,33 Of note, all chemotherapy-related decisions, including the type and number of cycles of induction and consolidation, were made before study entry, and investigators were not informed about MRD status during the study. Proportions of patients who received consolidation therapy were similar between the overall baseline MRD+ and MRD− subgroups, as was the number of consolidation cycles and the median total number of prior chemotherapy cycles (induction plus or minus consolidation) received; thus, the influence of prior chemotherapy on MRD status at baseline remains unclear. Consistent with previous reports, the presence of MRD during post-IC remission in the QUAZAR AML-001 study was strongly correlated with shorter time to AML relapse and poor survival, regardless of treatment assignment.4,22,26 In fact, baseline MRD status was an even stronger independent predictor of OS than randomized treatment in the multivariate analysis (Table 3). Nonetheless, oral-AZA substantially improved survival compared with placebo irrespective of baseline MRD status, and the survival benefit with oral-AZA relative to placebo was greater in the baseline MRD+ subgroup than in the MRD− subgroup. Multivariate analysis confirmed the significant independent treatment effect of oral-AZA vs placebo on OS and RFS when controlling for MRD status at baseline.
QUAZAR AML-001 is the first large randomized trial to show a substantially increased conversion rate from MRD+ to MRD− status with an active AML maintenance therapy: the rate of MRD response in the oral-AZA arm (37%) was nearly twice that in the placebo arm (19%), and median duration of MRD negativity on study was more than doubled with oral-AZA (11 vs 5 months, respectively). In multivariate analysis, oral-AZA was a significant independent predictor of achieving MRD response compared with placebo when controlling for cytogenetic risk and NPM1 status at diagnosis, number of consolidation cycles received, and baseline MRD percent. For patients with detectable MRD at baseline, achievement of MRD negativity (ie, MRD response) during oral-AZA treatment was associated with significantly improved survival. Although it seems intuitive that conversion from MRD positivity to MRD negativity is desirable and should correlate with better survival than sustained MRD positivity, this had not previously been confirmed in a prospective trial. Although the median time to MRD response was ∼2 months from randomization, and the majority of MRD responders in both treatment arms converted to MRD− status within the first 6 months on study, approximately one-fourth of the MRD responders treated with oral-AZA achieved MRD negativity after more than 6 months on study, suggesting a rationale for ongoing maintenance therapy.
The relative impact of faster vs slower MRD responses on OS and RFS is not clear. It is also unclear why there was a 19% MRD response rate in the placebo arm. Hypothetically, this could be attributable to residual effects of prior chemotherapy, but because the QUAZAR AML-001 trial is the first trial to collect serial, postremission MRD samples in an intensively treated older AML patient population, there is no benchmark of expected postchemotherapy MRD conversion rate to which the 19% observed in the placebo arm can be compared. It is unknown to what extent MRD conversion is intrinsic to a particular AML subtype (ie, a biological marker of chemotherapy sensitivity) vs influenced by subsequent consolidation chemotherapy and/or immunological factors. Also, in the QUAZAR AML-001 trial, patients were enrolled after they were already in remission and had received (or not received) consolidation chemotherapy. Thus, there are details related to the timing and doses of consolidation that are not available for consideration. In multivariate analysis, MRD responders in the placebo arm were more likely to have received a higher number of prestudy consolidation courses, whereas number of prestudy consolidation cycles was not significantly different among MRD responders in the oral-AZA arm.
Among patients who were MRD+ at baseline, those who achieved an MRD response during treatment were more likely to have received any consolidation than nonresponders, but there was no significant difference between MRD responders and those who remained MRD+ in the total number of prestudy chemotherapy cycles received. Also, among MRD responders, there was no clear correlation between the time since last dose of chemotherapy and time to achievement of MRD response on study. Finally, the duration of MRD negativity did not appear to be influenced by the number of prestudy consolidation cycles. For these analyses, MRD assessment was performed at 3-month intervals starting on cycle 3, day 1 (the first postbaseline MRD assessment) to minimize the requirement for invasive bone marrow aspirate collection. Thus, median time to conversion from MRD+ to MRD− was at ∼60 days (ie, at approximately cycle 3, day 1), and the median time between last MRD− assessment and relapse was estimated at ∼90 days (the duration between postbaseline MRD sampling assessments). Given the strong prognostic value of MRD status, less invasive approaches to MRD determination are desirable, but at this time, MRD solely from peripheral blood samples is not recommended.22
Though MRD detection in AML is rapidly evolving, with increasingly sensitive and specific technologies, there is no single, perfect MRD test yet in AML.25 Currently, the ideal approach to MRD detection may be to combine different testing modalities, including MFC, next-generation sequencing, and PCR.34 Still, mutation-specific sequencing approaches may not detect evolving, subclonal populations of cells lacking the known founder mutation,22 and rare subpopulations of normal/transitory cells in both bone marrow and peripheral blood may mimic MRD, complicating MRD assessment with MFC.35 Longitudinal molecular MRD assessments of patient samples in this study are currently under investigation but are challenging because the QUAZAR AML-001 trial included only patients in remission, a high proportion of whom (53%) were MRD− at baseline. Also, the trial began in 2010, when it was not yet standard of care to obtain comprehensive molecular genetic data at the time of AML diagnosis. Thus, customized platforms of deeper molecular detection (high gene coverages exceeding 5000×) and bioinformatics methods are required to optimize data filtering to derive the gene mutation calls. Importantly, irrespective of modality of assessment, it is clear that not all MRD− AML patients remain in remission, and not all MRD+ patients ultimately relapse. There is strong momentum within the AML treatment community toward developing internationally standardized MFC techniques (eg, antibody panel size, sample handling, instrumentation, data collection, leukemic stem cell identification) that may mitigate these limitations and increase the usefulness and comparability of MRD assessments.22,25,36
Overall, the longitudinal, MFC-based MRD analyses in QUAZAR AML-001 showed that, compared with placebo, older patients with AML in first remission who received maintenance treatment with oral-AZA had improved OS and RFS independent of MRD status at study entry were more likely to achieve MRD negativity and had a longer overall duration of MRD negativity. Persistence of MRD after IC was significantly and independently predictive of inferior outcomes, even after controlling for randomized treatment. Additional MRD assessments of QUAZAR AML-001 data are ongoing and may offer further insights into the impact of oral-AZA on suppression of residual leukemic clones in specific patient populations.
Acknowledgments
Editorial support on an early draft of the manuscript was provided by Brian Kaiser and Jason Rogers from Medical Communication Company, Inc. (Wynnewood, PA), funded by Bristol Myers Squibb Company, and in accordance with Good Publication Practice guidelines.
This study was sponsored and funded by Celgene Corporation, a Bristol Myers Squibb company.
Authorship
Contribution: The sponsors collected and analyzed data in conjunction with all authors; G.J.R. and H.D. collaborated on the first draft of the manuscript; and all authors revised the manuscript and reviewed and approved the final version for submission.
Conflict-of-interest disclosure: G.J.R. reports consultancy, advisory board, or data and safety monitoring committee for AbbVie, Actinium, Agios, Amgen, Astex, Astellas, AstraZeneca, Bayer, Blueprint Medicines, Bristol Myers Squibb, Celgene, Daiichi Sankyo, GlaxoSmithKline, Helsinn, Janssen, Jasper Therapeutics, Jazz, Mesoblast, MEI Pharma (IDMC Chair), Novartis, Otsuka, Pfizer, Roche/Genentech, Sandoz, and Takeda (IRC Chair); and research support from Cellectis and Janssen. F.R. reports honoraria and consulting fees from Bristol Myers Squibb and Celgene; and research funding from Bristol Myers Squibb. A.H.W. reports study-related fees and personal fees from Celgene; royalties from Walter and Eliza Hall Institute of Medical Research; grants from the Medical Research Future Fund; grants and personal fees from Servier, AbbVie, Novartis, Celgene, Astra Zeneca, and Janssen; and personal fees from Astellas, Pfizer, Macrogenics, and Amgen. H.D. reports personal fees from Amgen, Celgene, Pfizer, Incyte, Novartis, Jazz Pharma, Cellectis, Immunogen, Daiichi Sankyo, Sunesis, Astellas, Janssen, Servier, Shire-Baxalta, Abbvie, Otsuka, and Menarini; and grants from Amgen, Novartis, Pfizer, Jazz Pharma, Incyte, and Servier. F.T. reports study support from Bristol Myers Squibb and Celgene. M.T.V. reports honoraria from Roche and Celgene and research funding and speakers’ bureau participation for Celgene. A.C.S. reports clinical trial support from AbbVie, Agios, Amgen, Bristol Myers Squibb, GlycoMimetics, Kite, Loxo, Novartis, Pfizer, Servier; and advisory boards/honoraria from AbbVie, Agios, Amgen, Astellas, Bristol Myers Squibb, Jazz, Novartis, Pfizer, Taiho, and Teva. K.P. reports research funding and honorarium from Celgene and Novartis. I.L.T., B.S., J.Z., C.L.B., A.R., and D.L.M. report employment at and equity interest in Bristol Myers Squibb. G.O. reports research funding from Celgene, Novartis, Johnson & Johnson, and Genentech; and consultancy for Celgene, Roche, Johnson & Johnson, Agios, Jazz, Astellas, Daiichi Sankyo, Amgen, Novartis, and Genetech. H.D. reports personal fees from Abbvie, Agios, Astellas, Astex Pharmaceuticals, Helsinn, Janssen, Oxford Biomedicals, and Roche; grants and personal fees from Amgen, Celgene, Jazz Pharmaceuticals, and Novartis; and grants from AROG Pharmaceuticals, Bristol Myers Squibb, Pfizer, and Sunesis. I.L.T. is no longer employed at Celgene, a Bristol Myers Squibb Company.
Correspondence: Gail J. Roboz, Weill Cornell Medical College, 520 East 70th St, Starr Pavilion, 3rd Fl, New York, NY 10021; e-mail: gar2001@med.cornell.edu.
Bristol Myers Squibb policy on data sharing may be found at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal