

Background
Extranodal NK/T cell lymphoma (ENKTL) is rare in western countries but rather common in Asia and South America, characterized with Epstein-Barr virus (EBV) infection. Patients with advanced stage (III/IV) ENKTL has a poor survival and low response to conventional CHOP-like chemotherapy, with a 5-year overall survival rate of only 30%. Retrospective study showed that SMILE regimen had a certain effect on ENKTL, but the toxicity limited its further clinical application. More effective treatment regimens are required to be explored for systematic, prospective, controlled, randomized clinical trials. Recently, studies revealed that asparaginase-based combination chemotherapy such as P-Gmox(Pegaspargase, Gemcitabine, Oxaliplatin)is effective in patients of ENKTL. However standard treatment for newly untreated advanced ENKTL is still controversial. We developed a refined chemotherapeutic DDGP (dexamethasone, cisplatin, gemcitabline, and peg-asparaginase) regimen and proceeded a prospective randomized, multicenter and open-label clinical trial to evaluate and compare the efficacy and safety of DDGP with SMILE regimen in patients with newly diagnosed stage III/IV ENKTL in January 2011. Based on the encouraging interim results in 2016(Li, L et al.Clin Cancer Res, 2016), we presented the final results of this clinical investigation (ClinicalTrials.gov, No. NCT01501149).
Patients and methods:
The study was initiated at 9 centers in China in January 2011. Patients aged 14-70 with newly diagnosed ENKTL in stages III/IV, and ECOG performance score of 0-2 were enrolled. According to a computer-generated randomization schedule, eligible patients were assigned either DDGP regimen (cisplatin 20 mg/m² on day 1-4; dexamethasone 15mg/m2 on d1-5; gemcitabine 800mg/m2 on d1,8; pegaspargase 2500 IU/m2 on d1; 21 days per cycle)or SMILE regimen (methotrexate 2g/m2 on d1; dexamethasone 40mg/m2 on d2-4; ifosfamide 1500mg/m2 on d2-4; L-asparaginase 6000 U/m2 on d3-9; etoposide 100 mg/m2 on d2-4; 21 days per cycle) for up to 6 cycles unless disease progression, unacceptable toxicity or patient rejection. Efficacy was evaluated every two cycles. The primary endpoint was progression-free survival (PFS), and secondary endpoints included overall response rate (ORR) and overall survival (OS). In addition we compared the safety and tolerability between DDGP and SMILE regimens. The Kaplan-Merier method was used to evaluate for survival of freedom from events, and the log-rank test was used to evaluate differences among two groups.
Results:
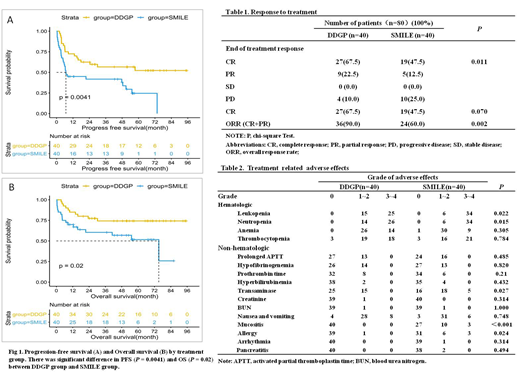
A total of 87 eligible newly diagnosed advanced ENKTL patients were randomly assigned for the study and 80 patients were included into intention-to-treat population (40 patients in DDGP group and 40 patients in SMILE group). Data were collected from January 2011 to February 2019. Baseline characteristics of the two group patients were well balanced. At median follow-up of 41.5 months, the median PFS and OS in the SMILE group were 6.83 months and 75.2 months, respectively, while the median PFS and OS in the DDGP group have not been reached (Fig 1). The 3-year PFS rate and 5-year OS rate in DDGP group were higher than in SMILE group (56.6% vs. 41.8% for 3-year PFS, P=0.004; 74.3% vs. 51.7% for 5-year OS, P=0.02). No difference of the complete remission (CR) rate was observed between two groups, while overall response rate (ORR) in DDGP group was higher than in SMILE group (90.0% vs. 60.0%, p=0.002) (Table 1). More frequently 3/4 grade hematologic toxicities such as leucopenia and netropenia were observed in SMILE group than in DDGP group (p=0.022, p=0.015). Non-hematologic toxicities included elevated transaminase, mucositis and allergy were higher in SMILE group than in DDGP group(p=0.027, p<0.001, p=0.024). Pancreatitis occurred in 2 patients in SMILE group, but not in DDGP group (Table 2). In addition, treatment-related deaths rate was up to 17.5% in SMILE regimen which was mainly caused by infection and hemorrhage due to bone marrow suppression. Such event was only 10% in DDGP regimen.
Conclusion: DDGP regimen produced prolonged survival, better tolerability and safety than SMILE regimen in newly diagnosed advanced ENKTL.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal