

Background: NK cells have the capacity to kill tumor targets, representing a novel immunotherapeutic approach to cancer. We have shown promising clinical activity in AML with a previous NK cell preparation. Limitations of NK therapies have included specificity, persistence after infusion, and potential for maximal activity of NK cells in vivo. GDA-201 is a cellular product composed of natural killer (NK) cells from healthy donors expanded ex vivo with nicotinamide (NAM) and IL-15; this is a unique ex vivo activation strategy to induce persistence of potent anti-tumor activity. Prior in vitro studies and pre-clinical models demonstrated that NAM-exposed NK cells exhibited augmented resistance against exhaustion and improved killing function, proliferation, and organ retention. We now report safety and efficacy from a phase 1 clinical trial of GDA-201 in patients (pts) with relapsed or refractory (R/R) NHL or MM.
Methods: Following donor apheresis, CD3-depleted mononuclear cells were cultured for 14-16 days with NAM (5mM) and IL-15 (20ng/ml), resulting in a 40-fold increase in NK cells and increased expression of CD62L from 2.9% to 21%. GDA-201 contained ~98% NK cells, and CD3 content was maintained at <0.5% (<5x105/kg/dose). Pts with R/R CD 20-positive NHL or refractory MM received cyclophosphamide (400mg/m2 IV x 3d) and fludarabine (30 mg/m2 /d IV x 3d), followed by two doses of GDA-201 (Days 0 and 2) and low-dose IL-2 (6 million units sc). Pts with NHL or MM received rituximab (375 mg/m2 x 4 weekly or elotuzumab (10 mg/kg x 3 weekly), respectively, to enhance NK cell targeting through antibody-dependent cellular cytotoxicity (ADCC).
Results: 20 pts were enrolled: 7 with NHL (4 follicular, 2 transformed, 1 diffuse large cell lymphoma) and 13 with MM, in 3 cohorts of escalating GDA-201 dose; 11 pts received the maximum target dose (median 1.7 x 108 cells/kg, range 1.6-2.0 x 108 cells/kg). There were no dose limiting toxicities. The most common grade 3/4 adverse events were neutropenia and thrombocytopenia, febrile neutropenia (n=2), increased creatinine, hyponatremia, pulmonary edema; all events were transient. One pt had grade 2 cytokine release syndrome at day 18, presenting with fever, hypoxemia and hypotension, responding to tocilizumab; pt later died of E Coli sepsis. There were no neurotoxic events, GVHD or marrow aplasia.
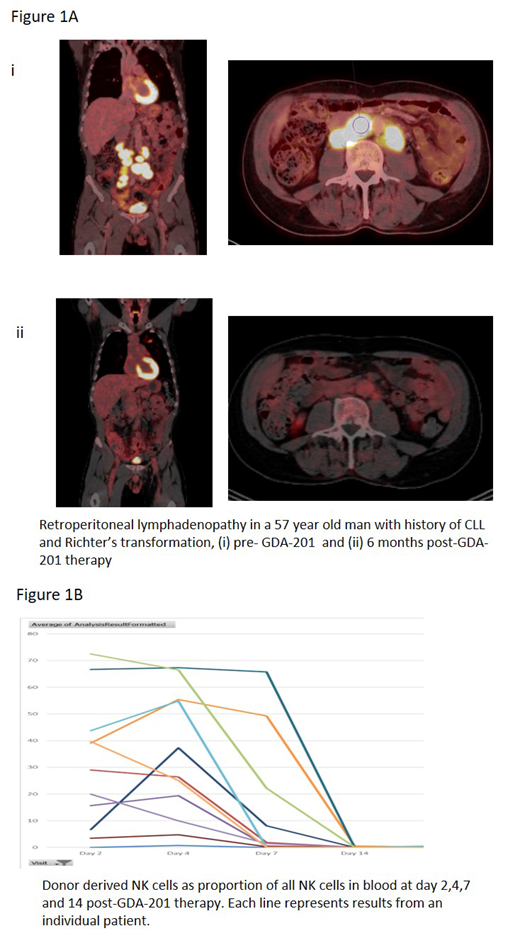
Among 7 NHL pts, there were 3 CR and 2 PR with overall response rate of 71%. Median duration of response was 12 months (CR patients) and 5 months (PR patients). Figure 1A illustrates a 57-year-old man with history of CLL and Richter's transformation (large cell lymphoma), pre- GDA-201 and 6 months post therapy; the pt had continued response with 80% tumor shrinkage at 6 months. In MM patients, 1 patient with extramedullary disease had CR and 4 had SD with median duration 2.5 months. In our previous study using overnight-activated NK cells, persistence 7 days after adoptive transfer was limited. Using GDA-201, flow cytometry confirmed persistence of donor NAM-NK in peripheral blood up to day 7-10 (day 7 range 2-55% donor NK cells; Figure 1B), as well as enhanced in vivo proliferation (median Ki67 99%).
Conclusions: Cellular therapy using GDA-201 with monoclonal antibodies was safe, and demonstrated early evidence of clinical activity in heavily pre-treated pts with advanced NHL and MM. The recommended dose of GDA-201 for phase 2 is 2.0 x 108 cells/kg. The clinical responses showed that NK cell targeting through ADCC can be efficacious and increase response. Laboratory studies showed that GDA-201 had better persistence than observed in our previous studies using overnight activated cytokine alone stimulated NK cells. This study demonstrated that GDA-201 has an efficacy signal, and larger phase II studies are warranted.
Bachanova:Incyte: Research Funding; Gamida Cell: Research Funding; Novartis: Research Funding; GT Biopharma: Research Funding; Celgene: Research Funding; Kite: Membership on an entity's Board of Directors or advisory committees; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees. McKenna:Fate Therapeutics: Research Funding; Magenta Therapeutics: Research Funding; CIBMTR BMT CTN (NIH): Other: Medical Monitor; Icahn School of Medicine, New York, New York: Consultancy; National Eye Institute (NIH): Other: DSMB (2); Gamida: Research Funding; NMDP: Other: Donor and Patient Safety Monitoring Advisory Group; Intima: Patents & Royalties: Royalities, Research Funding. Brachya:Gamida Cell: Employment, Equity Ownership. Peled:Gamida Cell: Employment, Equity Ownership. Miller:GT BioPharma: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; CytoSen: Membership on an entity's Board of Directors or advisory committees; Dr. Reddys Laboratory: Membership on an entity's Board of Directors or advisory committees; Moderna: Membership on an entity's Board of Directors or advisory committees; Fate Therapeutics, Inc: Consultancy, Research Funding; OnKImmune: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal